

First-year lymphocyte T CD4+ response to antiretroviral therapy according to the HIV type in the IeDEA West Africa collaboration
- PMID: 20397306
- PMCID: PMC2880184
- DOI: 10.1097/qad.0b013e3283377a06
First-year lymphocyte T CD4+ response to antiretroviral therapy according to the HIV type in the IeDEA West Africa collaboration
Abstract
Objective: To compare the lymphocyte T CD4+ (CD4) response to combinations of antiretroviral therapy (ART) in HIV-1, HIV-2 and dually positive patients in West Africa.
Design and setting: Collaboration of 12 prospective cohorts of HIV-infected adults followed in Senegal (2), Gambia (1), Mali (2), Benin (1) and Côte d'Ivoire (6).
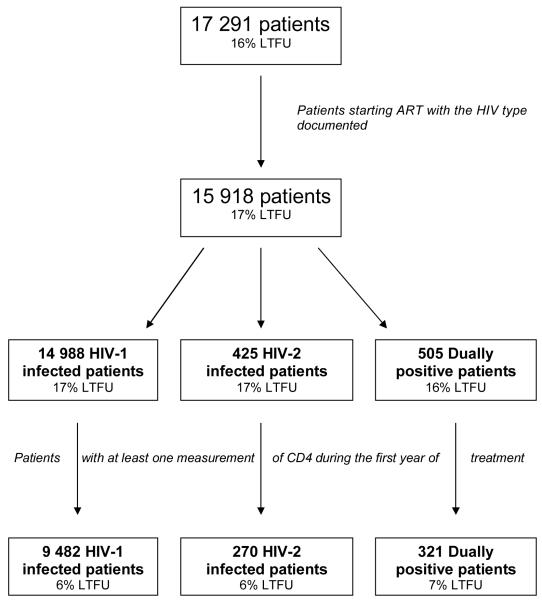
Subjects: Nine thousand, four hundred and eighty-two patients infected by HIV-1 only, 270 by HIV-2 only and 321 dually positive, who initiated an ART.
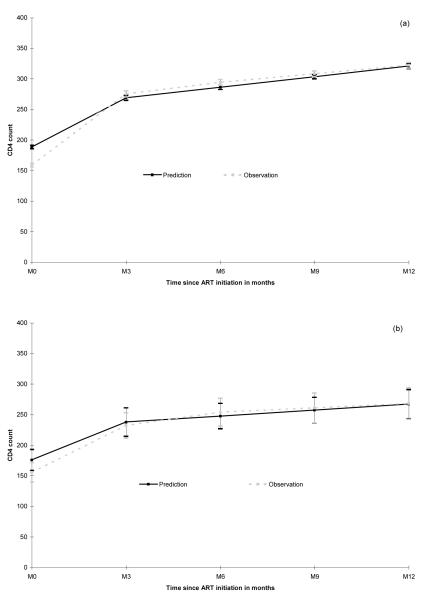
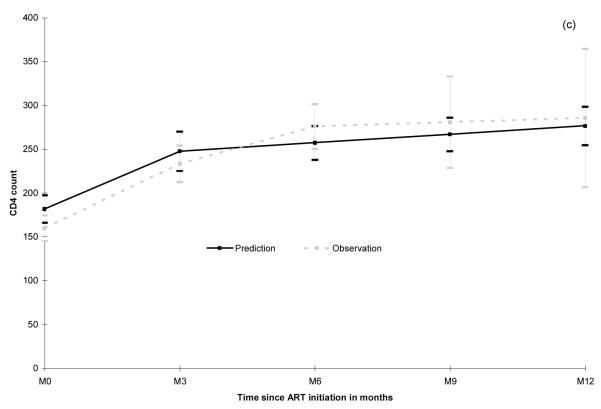
Outcome measures: CD4 change over a 12-month period.
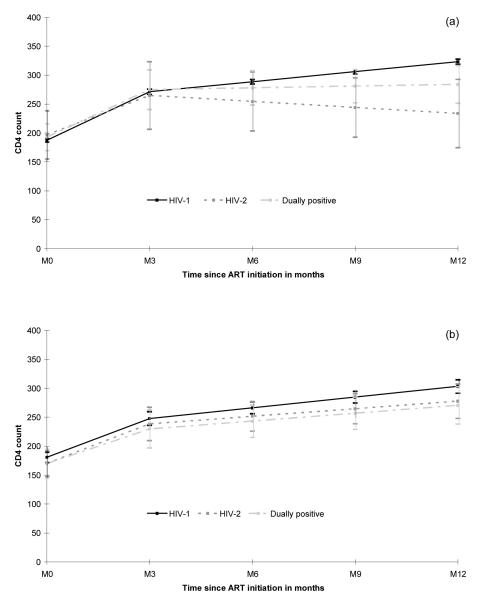
Results: Observed CD4 cell counts at treatment initiation were similar in the three groups [overall median 155, interquartile range (IQR) 68; 249 cells/microl). In HIV-1 patients, the most common ART regimen was two nucleoside reverse transcriptase inhibitors (NRTIs) and one non-nucleoside reverse transcriptase inhibitor (NNRTI; N = 7714) as well as for dually positive patients (N = 135). HIV-2 patients were most often treated with a protease inhibitor-based regimen (N = 193) but 45 of them were treated with an NNRTI-containing ART. In those treated with a NNRTI-containing regimen, the estimated mean CD4 change between 3 and 12 months was significantly lower in HIV-2 (-41 cells/microl per year) and dually positive patients (+12 cells/microl per year) compared to HIV-1 patients (+69 cells/microl per year, overall P value 0.01). The response in HIV-2 and dually positive patients treated by another regimen (triple NRTIs or protease inhibitor-containing ART) was not significantly different than the response obtained in HIV-1-only patients (all P values >0.30).
Conclusion: An optimal CD4 response to ART in West Africa requires determining HIV type prior to initiation of antiretroviral drugs. NNRTIs are the mainstay of first-line ART in West Africa but are not adapted to the treatment of HIV-2 and dually positive patients.
Figures
References
-
- World Health Organization Towards universal access: scaling up priority HIV/AIDS interventions in the health sector: progress report 2008. Geneva: 2008.
-
- van der Loeff MF, Awasana AA, Sarge-Njie R, van der Sande M, Jaye A, Sabally S, et al. Sixteen years of HIV surveillance in a West African research clinic reveals divergent epidemic trends of HIV-1 and HIV-2. International Journal of Epidemiology. 2006;35:1322–1328. - PubMed
-
- Eholie S, Anglaret X. Commentary: Decline of HIV-2 prevalence in West Africa: good news or bad news? International Journal of Epidemiology. 2006;35:1329–1330. - PubMed
-
- Valadas E, Franca L, Sousa S, Antunes F. 20 Years of HIV-2 Infection in Portugal: Trends and Changes in Epidemiology. Clinical Infectious Diseases. 2009;48:1166–1167. - PubMed
-
- Whittle H, Morris J, Todd J, Corrah T, Sabally S, Bangali J, et al. HIV-2-infected patients survive longer than HIV-1-infected patients. AIDS. 1994;8:1617–1620. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
