

Inter-rater reliability of the Full Outline of UnResponsiveness score and the Glasgow Coma Scale in critically ill patients: a prospective observational study
- PMID: 20398274
- PMCID: PMC2887186
- DOI: 10.1186/cc8963
Inter-rater reliability of the Full Outline of UnResponsiveness score and the Glasgow Coma Scale in critically ill patients: a prospective observational study
Abstract
Introduction: The Glasgow Coma Scale (GCS) is the most widely used scoring system for comatose patients in intensive care. Limitations of the GCS include the impossibility to assess the verbal score in intubated or aphasic patients, and an inconsistent inter-rater reliability. The FOUR (Full Outline of UnResponsiveness) score, a new coma scale not reliant on verbal response, was recently proposed. The aim of the present study was to compare the inter-rater reliability of the GCS and the FOUR score among unselected patients in general critical care. A further aim was to compare the inter-rater reliability of neurologists with that of intensive care unit (ICU) staff.
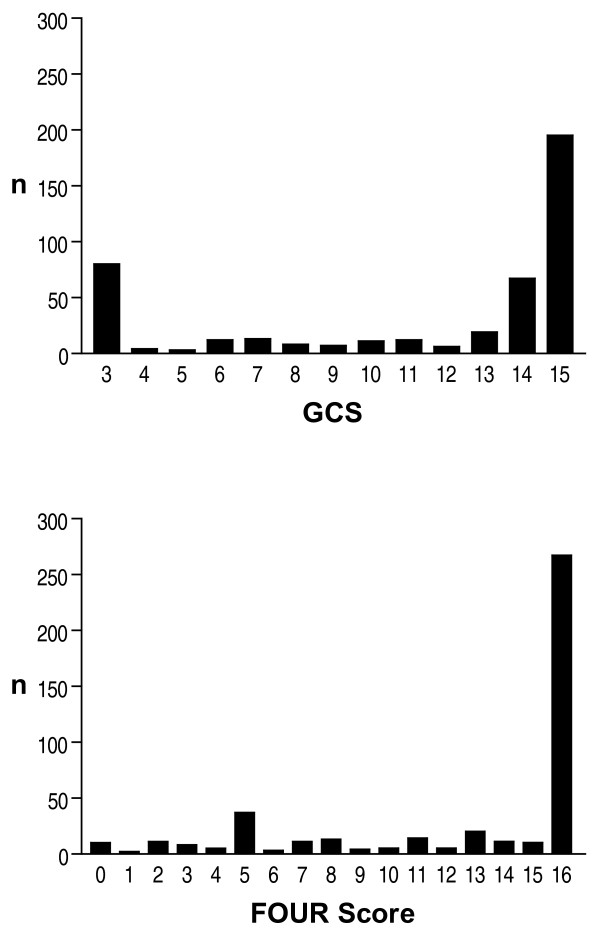
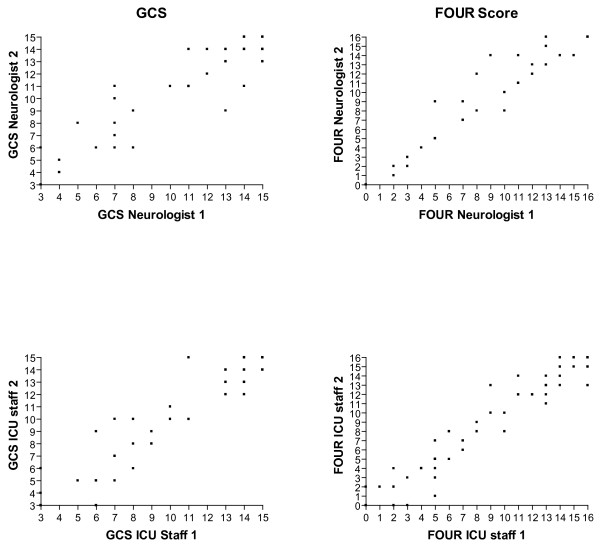
Methods: In this prospective observational study, scoring of GCS and FOUR score was performed by neurologists and ICU staff on 267 consecutive patients admitted to intensive care.
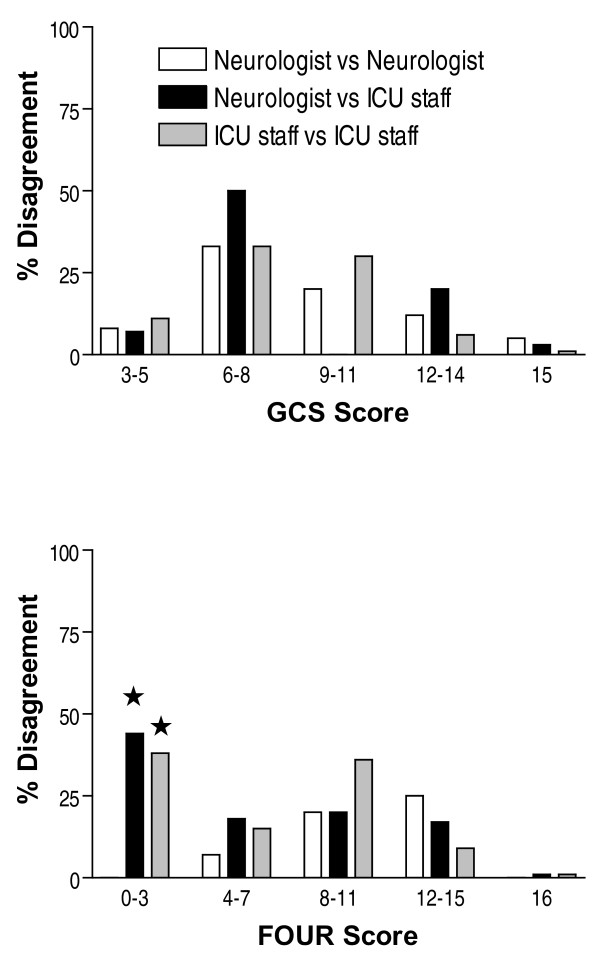
Results: In a total of 437 pair wise ratings the exact inter-rater agreement for the GCS was 71%, and for the FOUR score 82% (P = 0.0016); the inter-rater agreement within a range of +/- 1 score point for the GCS was 90%, and for the FOUR score 92% (P = ns.). The exact inter-rater agreement among neurologists was superior to that among ICU staff for the FOUR score (87% vs. 79%, P = 0.04) but not for the GCS (73% vs. 73%). Neurologists and ICU staff did not significantly differ in the inter-rater agreement within a range of +/- 1 score point for both GCS (88% vs. 93%) and the FOUR score (91% vs. 88%).
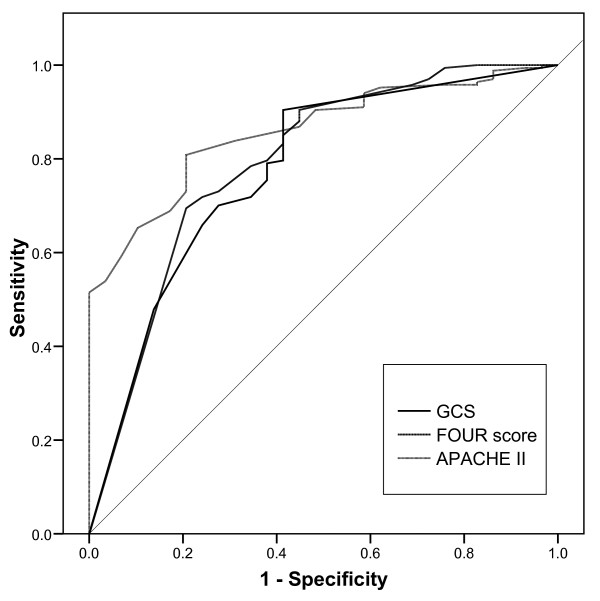
Conclusions: The FOUR score performed better than the GCS for exact inter-rater agreement, but not for the clinically more relevant agreement within the range of +/- 1 score point. Though neurologists outperformed ICU staff with regard to exact inter-rater agreement, the inter-rater agreement of ICU staff within the clinically more relevant range of +/- 1 score point equalled that of the neurologists. The small advantage in inter-rater reliability of the FOUR score is most likely insufficient to replace the GCS, a score with a long tradition in intensive care.
Figures
Similar articles
-
A multicenter prospective study of interobserver agreement using the Full Outline of Unresponsiveness score coma scale in the intensive care unit.Crit Care Med. 2012 Sep;40(9):2671-6. doi: 10.1097/CCM.0b013e318258fd88. Crit Care Med. 2012. PMID: 22732282
-
Validity of the FOUR score coma scale in the medical intensive care unit.Mayo Clin Proc. 2009 Aug;84(8):694-701. doi: 10.4065/84.8.694. Mayo Clin Proc. 2009. PMID: 19648386 Free PMC article.
-
Validation of the Full Outline of Unresponsiveness (FOUR) Scale for conscious state in the emergency department: comparison against the Glasgow Coma Scale.Emerg Med J. 2011 Jun;28(6):486-90. doi: 10.1136/emj.2009.085845. Epub 2010 Oct 13. Emerg Med J. 2011. PMID: 20943845
-
Evaluation of coma: a critical appraisal of popular scoring systems.Neurocrit Care. 2011 Feb;14(1):134-43. doi: 10.1007/s12028-010-9409-3. Neurocrit Care. 2011. PMID: 20652445 Review.
-
The current significance of the FOUR score: A systematic review and critical analysis of the literature.J Neurol Sci. 2020 Feb 15;409:116600. doi: 10.1016/j.jns.2019.116600. Epub 2019 Nov 27. J Neurol Sci. 2020. PMID: 31811988
Cited by
-
The Relationship of the FOUR Score to Patient Outcome: A Systematic Review.J Neurotrauma. 2019 Sep 1;36(17):2469-2483. doi: 10.1089/neu.2018.6243. Epub 2019 Jun 6. J Neurotrauma. 2019. PMID: 31044668 Free PMC article.
-
A comparison of the glasgow coma scale score with full outline of unresponsiveness scale to predict patients' traumatic brain injury outcomes in intensive care units.Crit Care Res Pract. 2014;2014:289803. doi: 10.1155/2014/289803. Epub 2014 Jun 10. Crit Care Res Pract. 2014. PMID: 25013727 Free PMC article.
-
FOUR Score Predicts Early Outcome in Patients After Traumatic Brain Injury.Neurocrit Care. 2017 Apr;26(2):225-231. doi: 10.1007/s12028-016-0326-y. Neurocrit Care. 2017. PMID: 27873233
-
Comparison of full outline of unresponsiveness score and Glasgow Coma Scale in Medical Intensive Care Unit.Ann Card Anaesth. 2019 Apr-Jun;22(2):143-148. doi: 10.4103/aca.ACA_25_18. Ann Card Anaesth. 2019. PMID: 30971594 Free PMC article.
-
Behavioral Assessment of Patients with Disorders of Consciousness.Semin Neurol. 2022 Jun;42(3):249-258. doi: 10.1055/s-0042-1756298. Epub 2022 Sep 13. Semin Neurol. 2022. PMID: 36100225 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
