

A phase I clinical study of high dose ketoconazole plus weekly docetaxel for metastatic castration resistant prostate cancer
- PMID: 20399458
- PMCID: PMC3474294
- DOI: 10.1016/j.juro.2010.02.020
A phase I clinical study of high dose ketoconazole plus weekly docetaxel for metastatic castration resistant prostate cancer
Abstract
Purpose: This phase I study of high dose ketoconazole and docetaxel was designed against castration resistant prostate cancer to determine the maximum tolerated doses, side effects, and pharmacokinetic interaction of co-administered docetaxel and ketoconazole.
Materials and methods: Patients with metastatic castration resistant prostate cancer received weekly docetaxel for 3 of every 4 weeks plus daily ketoconazole. Pharmacokinetic studies were performed on day 1 (docetaxel alone) and day 16 (after ketoconazole).
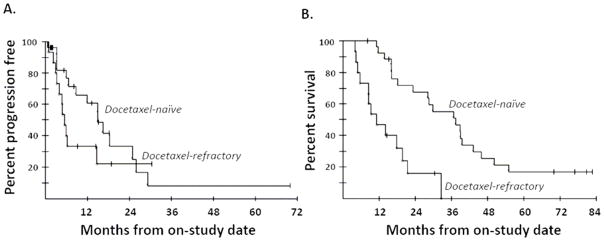
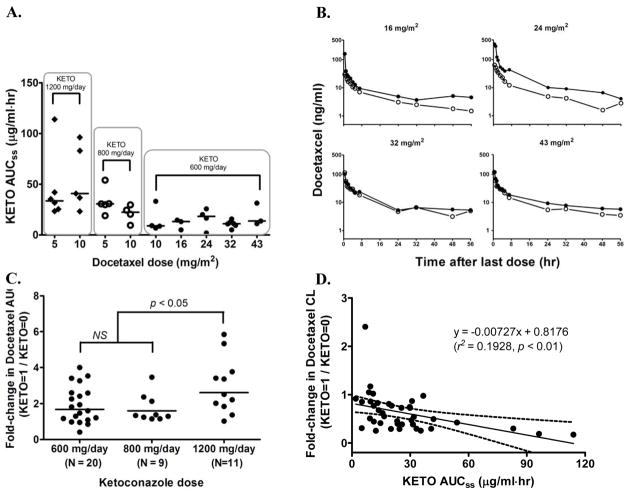
Results: The study enrolled 42 patients at 9 different dose levels. The combination regimens investigated included docetaxel weekly, increasing from 5 to 43 mg/m(2), with starting doses of 600, 800 or 1,200 mg ketoconazole daily. Decreases in prostate specific antigen of 50% or greater were seen in 62% of patients. Of 25 patients with soft tissue disease 7 (28%) had a partial response. Median overall survival was 22.8 months and was significantly greater in docetaxel naïve patients than in patients pretreated with docetaxel (36.8 vs 10.3 months, p = 0.0001). The most frequently observed adverse events were anemia, edema, fatigue, diarrhea, nausea, sensory neuropathy and elevated liver function tests. The fractional change in docetaxel clearance correlated significantly with ketoconazole exposure (p <0.01). Concomitant ketoconazole increased docetaxel exposure 2.6-fold with 1,200 mg daily, 1.6-fold with 800 mg daily and approximately 1.3 to 1.5-fold with 600 mg daily.
Conclusions: Combination regimens using 600 mg ketoconazole daily were fairly well tolerated and the maximum tolerated dose of docetaxel was 32 mg/m(2). Results suggest that the combination has significant antitumor activity in castration resistant prostate cancer. The long survival in the docetaxel naïve cohort warrants additional, larger trials of docetaxel with ketoconazole or possibly CYP17A1 inhibitors such as abiraterone.
Copyright 2010 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Smith BD, Smith GL, Hurria A, Hortobagyi GN, Buchholz TA. Future of cancer incidence in the United States: burdens upon an aging, changing nation. J Clin Oncol. 2009;27:2758–65. - PubMed
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Damber JE, Aus G. Prostate cancer. Lancet. 2008;371:1710–21. - PubMed
-
- Petrylak DP, Tangen CM, Hussain MH, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351:1513–20. - PubMed
-
- Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
