

Positive surgical margins at radical prostatectomy predict prostate cancer specific mortality
- PMID: 20399459
- PMCID: PMC2903223
- DOI: 10.1016/j.juro.2010.02.017
Positive surgical margins at radical prostatectomy predict prostate cancer specific mortality
Abstract
Purpose: Positive surgical margins in men undergoing radical prostatectomy for prostate cancer are associated with an increased risk of biochemical recurrence. Few data are available on the role of positive surgical margins in prostate cancer specific mortality. Using a large, population based national cancer registry we evaluated the risk of prostate cancer specific mortality associated with margin status.
Materials and methods: The SEER cancer registry data for patients diagnosed between 1998 and 2006 were used to identify men undergoing radical prostatectomy for prostate cancer. Margin status, pathological stage, Gleason grade and postoperative radiation therapy were recorded along with demographic data. Multivariate Cox regression analysis was used to estimate the risk of prostate cancer specific mortality associated with positive surgical margins.
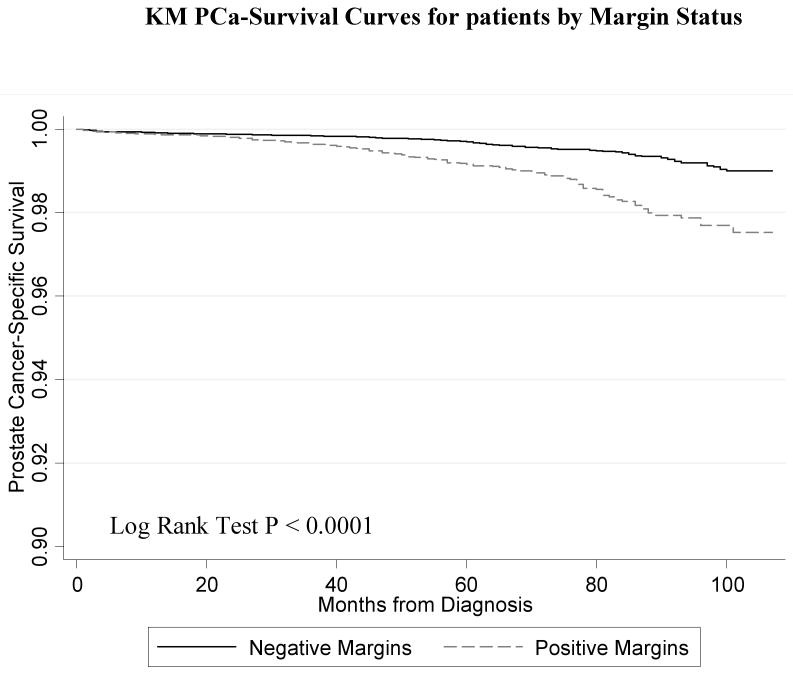
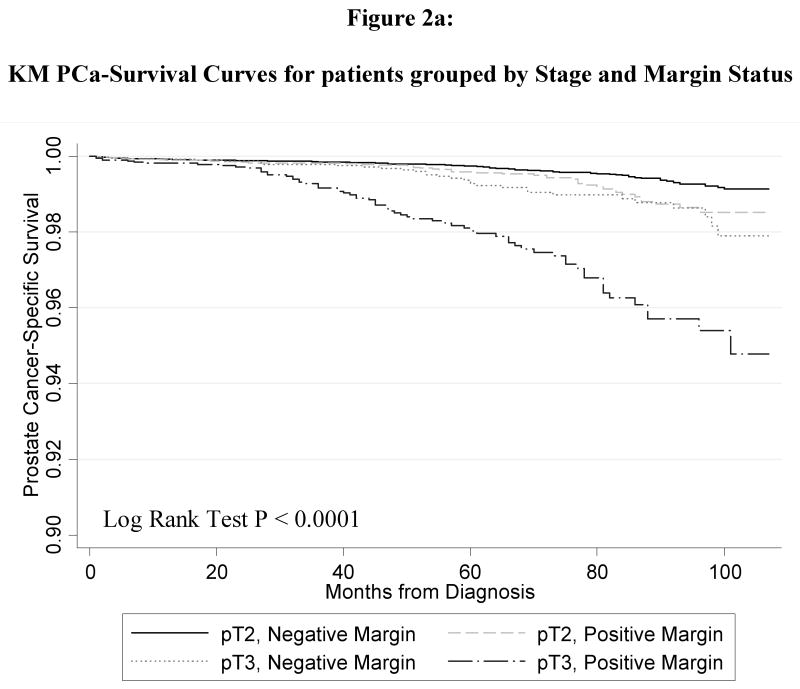
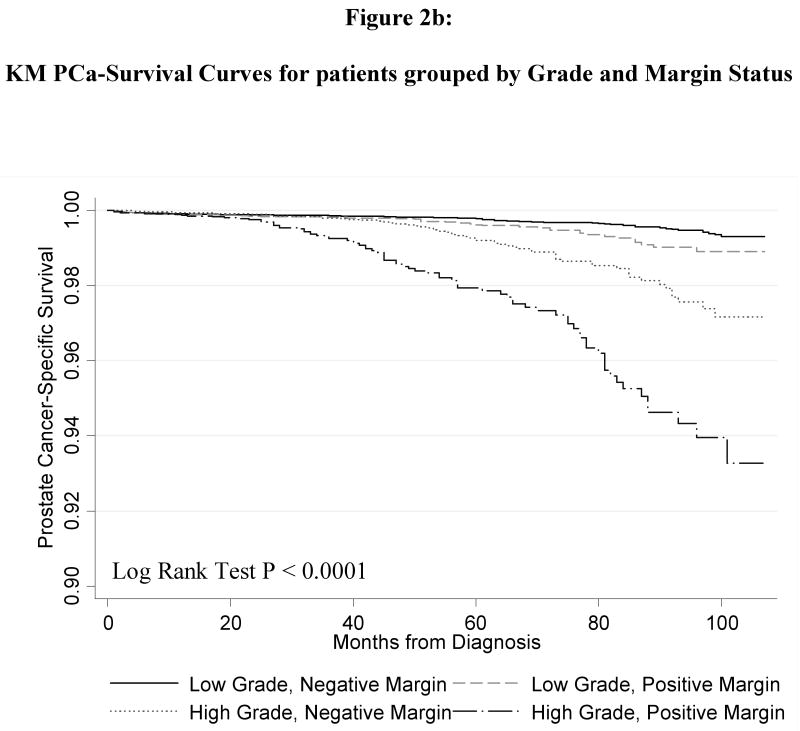
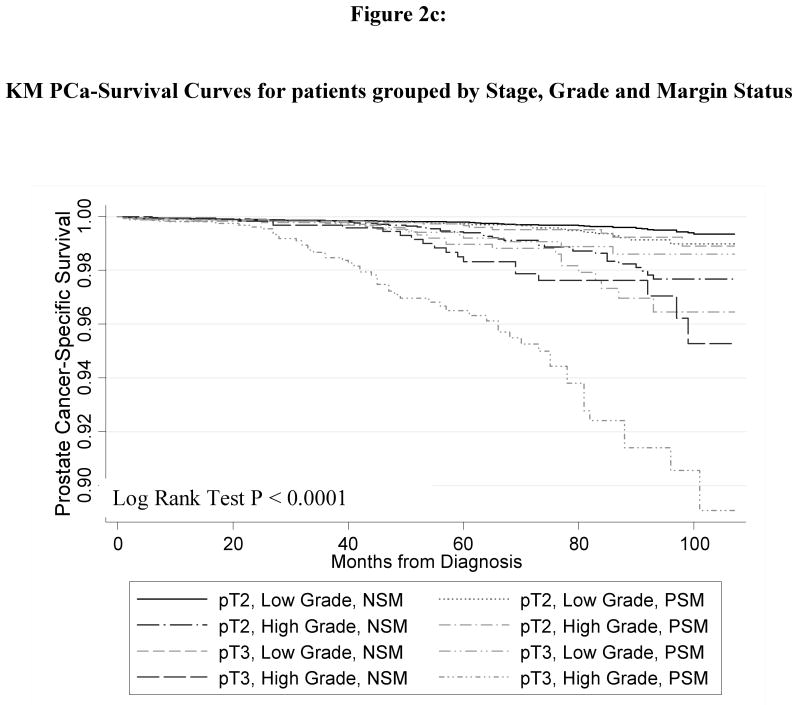
Results: A total of 65,633 patients comprised the cohort in which 291 (0.44%) prostate cancer specific deaths occurred during an average followup of 50 months. Positive surgical margins were reported in 21.2% of cases and were more common in pT3a than pT2 tumors (44% vs 18%, p <0.001) and higher grade tumors (28% vs 18%, p <0.001). The 7-year disease specific survival rates for those at highest risk for prostate cancer specific mortality (higher grade pT3a) were 97.6% for cases with negative surgical margins and 92.4% for those with positive surgical margins. Positive surgical margins were associated with a 2.6-fold increased unadjusted risk of prostate cancer specific mortality (HR 2.55, 95% CI 2.02-3.21). Positive surgical margins remained an independent predictor of prostate cancer specific mortality on multivariate analysis (HR 1.70, 95% CI 1.32-2.18).
Conclusions: These data demonstrate the independent role of positive surgical margins in prostate cancer specific mortality. These findings support the importance of optimizing surgical techniques to achieve a sound oncological surgical outcome with negative surgical margins when possible.
Copyright 2010 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Surgical margins following urological cancer surgery and clinical outcomes--does the United States need regional centralization of cancer care?J Urol. 2010 Jun;183(6):2126-7. doi: 10.1016/j.juro.2010.03.049. J Urol. 2010. PMID: 20399470 No abstract available.
References
-
- Cooperberg MR, Pasta DJ, Elkin EP, Litwin MS, Latini DM, Du Chane J, et al. The University of California, San Francisco Cancer of the Prostate Risk Assessment score: a straightforward and reliable preoperative predictor of disease recurrence after radical prostatectomy. J Urol. 2005;173(6):1938–42. - PMC - PubMed
-
- Freedland SJ, Amling CL, Dorey F, Kane CJ, Presti JC, Jr, Terris MK, et al. Race as an outcome predictor after radical prostatectomy: results from the Shared Equal Access Regional Cancer Hospital (SEARCH) database. Urology. 2002;60(4):670–4. - PubMed
-
- Suardi N, Porter CR, Reuther AM, Walz J, Kodama K, Gibbons RP, et al. A nomogram predicting long-term biochemical recurrence after radical prostatectomy. Cancer. 2008;112(6):1254–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
