

Prediction of vancomycin pharmacodynamics in children with invasive methicillin-resistant Staphylococcus aureus infections: a Monte Carlo simulation
- PMID: 20399990
- PMCID: PMC3097025
- DOI: 10.1016/j.clinthera.2010.03.005
Prediction of vancomycin pharmacodynamics in children with invasive methicillin-resistant Staphylococcus aureus infections: a Monte Carlo simulation
Abstract
Background: Due to the emergence of community-associated strains, the prevalence of invasive methicillin-resistant Staphylococcus aureus (MRSA) infections has increased substantially in pediatric patients. A vancomycin AUC(0-24)/MIC index >400 best predicts treatment outcomes for invasive MRSA infection in adults. Data on whether recommended vancomycin doses in children achieve this break point are lacking.
Objective: This study aimed to assess the likelihood that currently recommended vancomycin doses in children achieve AUC(0-24)/MIC >400.
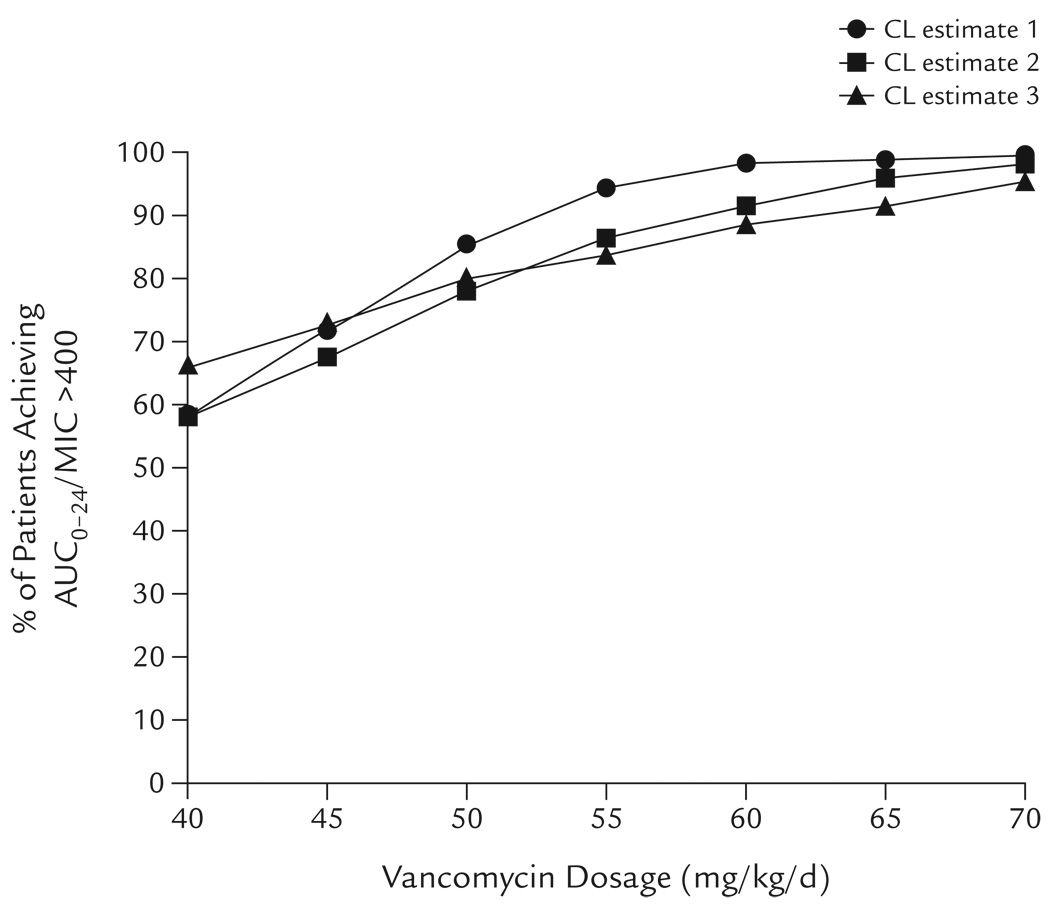
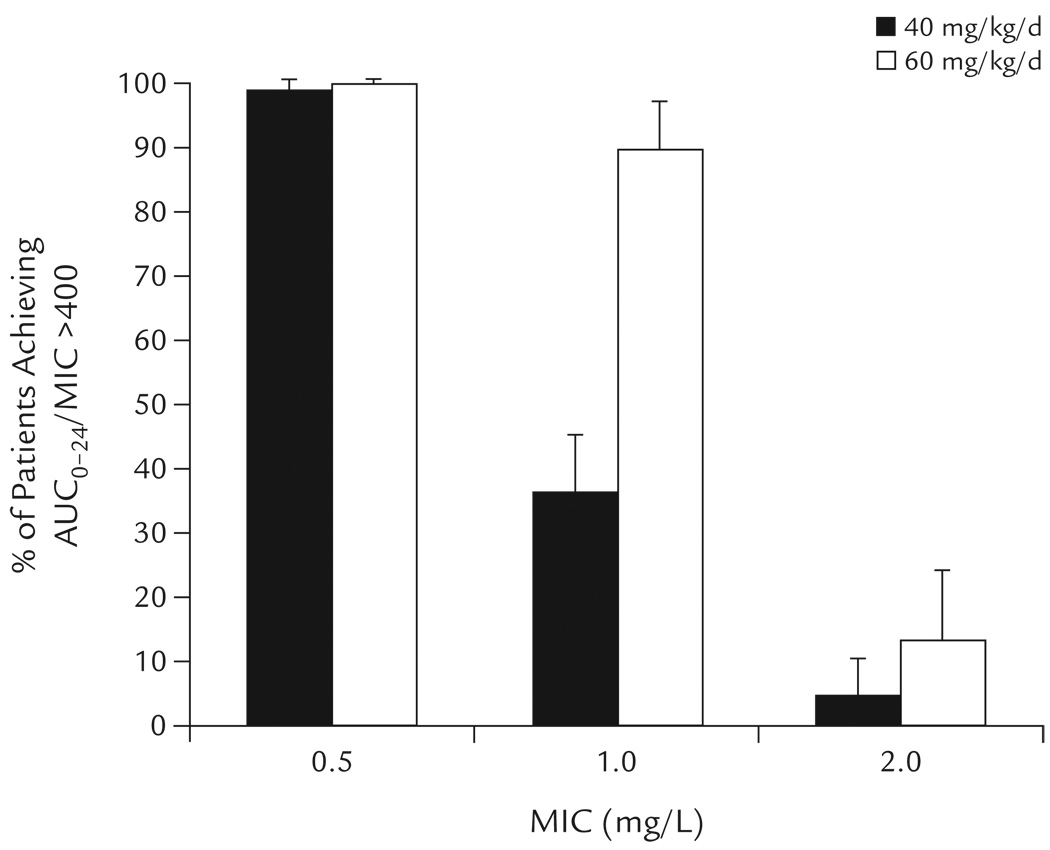
Methods: Vancomycin AUC(0-24)/MIC predictions were conducted across a range of dosages (40-70 mg/kg/d) using a Monte Carlo simulation (n = 5000). AUC(0-24) was calculated as daily dose divided by vancomycin clearance, and daily dose was fixed for a given simulation. Three literature-reported estimates in children were used to define vancomycin clearance and its variance. For the MIC distribution of MRSA isolates, susceptibility data were obtained from the University of California, San Francisco Children's Hospital, San Francisco, California (n = 180; 40% < or =0.5 mg/L; 59% = 1 mg/L; and 1% = 2 mg/L).
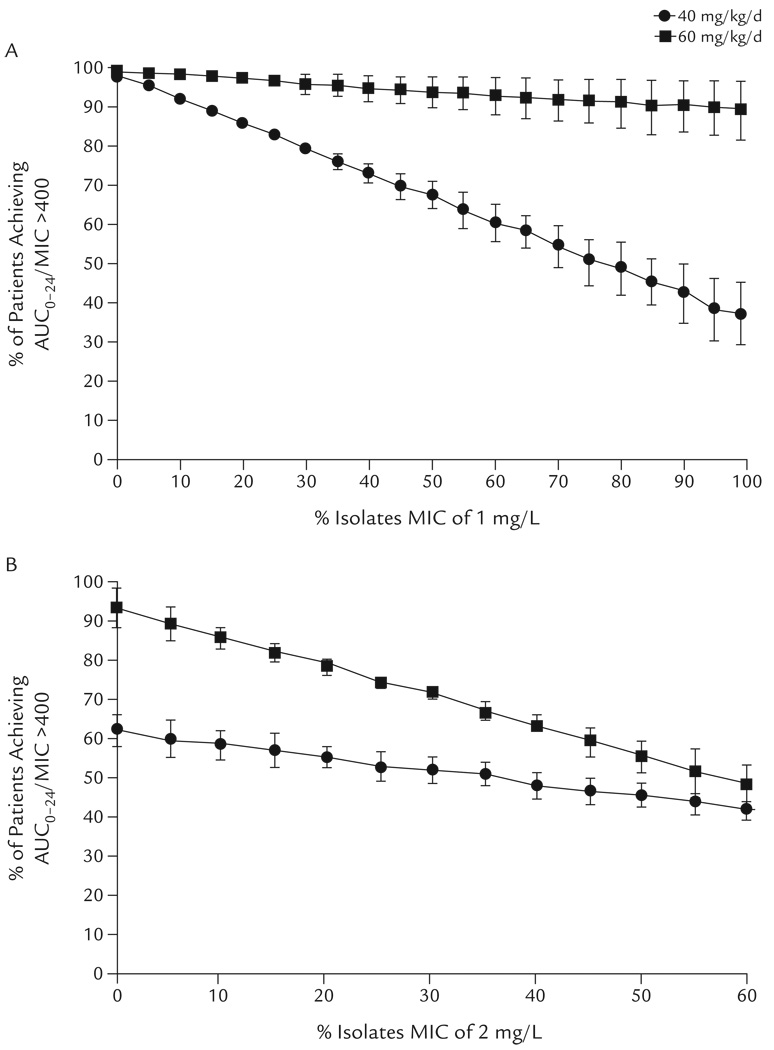
Results: Using the recommended empiric dosage of 40 mg/kg/d, 58% to 66% of children were predicted to achieve AUC(0-24)/MIC >400. Increasing the vancomycin dosage to 60 mg/kg/d substantially increased the likelihood (88%-98%) of achieving this pharmacodynamic target. On sensitivity analysis, a dosage of 40 mg/kg/d was more strongly influenced by small changes in MIC compared with 60 mg/kg/d.
Conclusions: Recommended empiric vancomycin dosing in children (40 mg/kg/d) was not predicted to consistently achieve the pharmacodynamic target of AUC(0-24)/MIC >400 for invasive MRSA infections. A vancomycin dosage of 60 mg/kg/d was predicted to optimize achievement of this target in children.
Copyright 2010 Excerpta Medica Inc. All rights reserved.
Conflict of interest statement
The authors have indicated that they have no other conflicts of interest regarding the content of this article.
Figures
References
-
- Vancocin (vancomycin injection) [package insert] Deerfield, Ill: Baxter Healthcare Corporation; 2003.
-
- Robertson J, Shilkofski N, editors. The Harriet Lane Handbook: A Manual for Pediatric House Officers. 17th ed. Philadelphia, Pa: Mosby; 2005.
-
- Taketomo CK, Hodding JH, Kraus DM. Lexi Comp’s Pediatric Dosage Handbook with International Trade Names Index: Including Neonatal Dosing, Drug Administration, & Extemporaneous Preparations (Lexi-Comp’s Drug Reference Handbooks) 14th ed. Hudson, Oh: Lexi-Comp; 2007.
-
- Long SS, Pickering LK, Prober CG, editors. Principles and Practice of Pediatric Infectious Diseases. 3rd ed. Philadelphia, Pa: Churchill Livingstone Elsevier; 2008.
-
- Schaad UB, McCracken GH, Jr, Nelson JD. Clinical pharmacology and efficacy of vancomycin in pediatric patients. J Pediatr. 1980;96:119–126. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
