

The pain imaging revolution: advancing pain into the 21st century
- PMID: 20400714
- PMCID: PMC3370428
- DOI: 10.1177/1073858409349902
The pain imaging revolution: advancing pain into the 21st century
Abstract
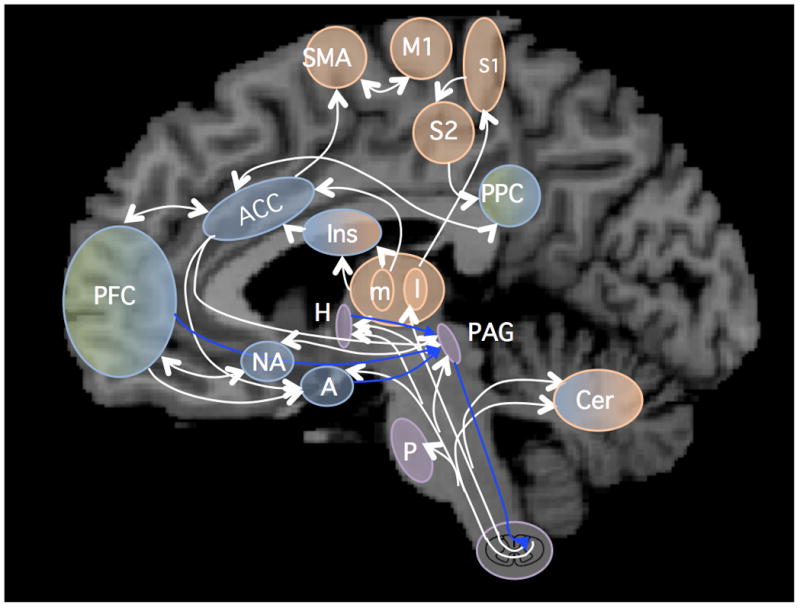
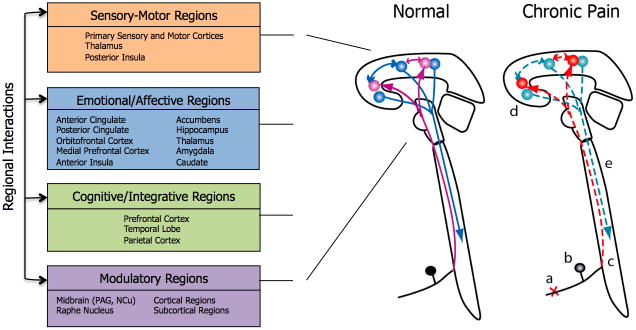
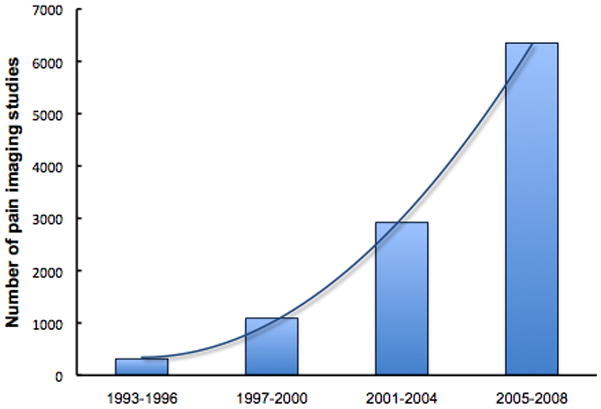
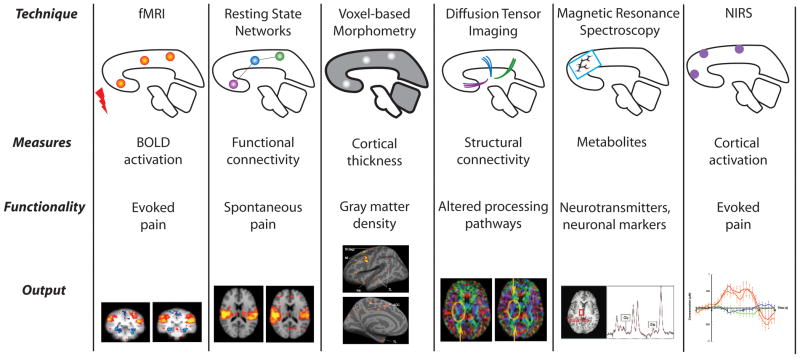
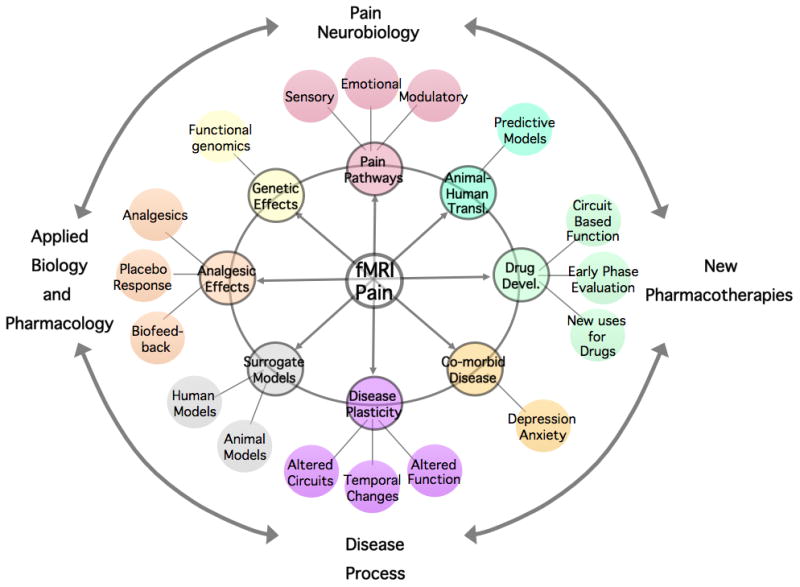
The great advances in brain imaging techniques over the last few decades have determined a shift in our understanding of chronic pain conditions and opened the door for new opportunities to develop better diagnoses and perhaps better drug treatments. Neuroimaging has helped shape the concept of chronic pain from a disease affecting mainly the somatosensory system, to a condition in which emotional, cognitive, and modulatory areas of the brain are affected, in addition to degenerative processes. All these contribute to the development and maintenance of pain symptoms and comorbid features, including alterations in anxiety, depression, and cognitive processes. In this article the authors review the current understanding of the brain changes in chronic pain and the developments made possible by the use of various brain imaging techniques. They also discuss the possible applications of brain imaging to developing a "pain phenotype" that could aid in diagnostic and treatment choices of chronic pain conditions.
Figures
Similar articles
-
Neuroimaging of pain: advances and future prospects.J Pain. 2008 Jul;9(7):567-79. doi: 10.1016/j.jpain.2008.02.008. Epub 2008 May 2. J Pain. 2008. PMID: 18455479 Review.
-
Neuroimaging: visualising the brain in pain.Neurol Sci. 2007 May;28 Suppl 2:S101-7. doi: 10.1007/s10072-007-0760-x. Neurol Sci. 2007. PMID: 17508154 Review.
-
Neuroimaging as a tool for pain diagnosis and analgesic development.Neurotherapeutics. 2009 Oct;6(4):755-60. doi: 10.1016/j.nurt.2009.08.003. Neurotherapeutics. 2009. PMID: 19789078 Free PMC article.
-
Cognitive neuroscience: origins and promise.Psychol Bull. 2000 Nov;126(6):873-89. doi: 10.1037/0033-2909.126.6.873. Psychol Bull. 2000. PMID: 11107880 Review.
-
Human brain mechanisms of pain perception and regulation in health and disease.Eur J Pain. 2005 Aug;9(4):463-84. doi: 10.1016/j.ejpain.2004.11.001. Epub 2005 Jan 21. Eur J Pain. 2005. PMID: 15979027 Review.
Cited by
-
Unraveling the Complex Web of Fibromyalgia: A Narrative Review.Medicina (Kaunas). 2024 Feb 4;60(2):272. doi: 10.3390/medicina60020272. Medicina (Kaunas). 2024. PMID: 38399559 Free PMC article. Review.
-
Getting the pain you expect: mechanisms of placebo, nocebo and reappraisal effects in humans.Nat Med. 2010 Nov;16(11):1277-83. doi: 10.1038/nm.2229. Epub 2010 Oct 14. Nat Med. 2010. PMID: 20948533
-
Molecular Aspects of Regional Pain Syndrome.Pain Res Manag. 2020 Apr 11;2020:7697214. doi: 10.1155/2020/7697214. eCollection 2020. Pain Res Manag. 2020. PMID: 32351641 Free PMC article. Review.
-
"ABC"-The Awareness-Body-Chart: A new tool assessing body awareness.PLoS One. 2017 Oct 16;12(10):e0186597. doi: 10.1371/journal.pone.0186597. eCollection 2017. PLoS One. 2017. PMID: 29036217 Free PMC article.
-
Structural brain alterations in patients with lumbar disc herniation: a preliminary study.PLoS One. 2014 Mar 3;9(3):e90816. doi: 10.1371/journal.pone.0090816. eCollection 2014. PLoS One. 2014. PMID: 24595036 Free PMC article.
References
-
- Apkarian AV, Bushnell MC, Treede RD, Zubieta JK. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain. 2005;9(4):463–84. - PubMed
-
- Apkarian AV, Krauss BR, Fredrickson BE, Szeverenyi NM. Imaging the pain of low back pain: functional magnetic resonance imaging in combination with monitoring subjective pain perception allows the study of clinical pain states. Neurosci Lett. 2001;299(1–2):57–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
