

Acute compartment syndrome in children: a case series in 24 patients and review of the literature
- PMID: 20401657
- PMCID: PMC3066331
- DOI: 10.1007/s00264-010-1016-6
Acute compartment syndrome in children: a case series in 24 patients and review of the literature
Abstract
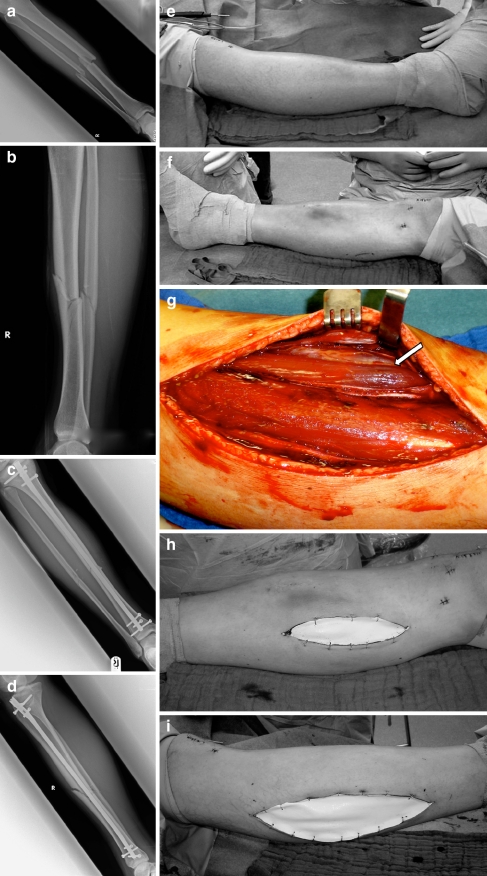
Trauma-associated acute compartment syndrome (ACS) of the extremities is a well-known complication in adults. There are only a handful of articles that describe the symptoms, the diagnostic procedure and treatment of ACS in children. The aim of this study was to analyse the diagnostic procedures in children compared to adolescents with ACS to obtain evidence for the diagnosis, treatment and outcome of children with ACS. Twenty-four children and adolescents with ACS have been treated at the Department of Trauma Surgery of the Medical University of Vienna, Austria. Two age-related groups were investigated to compare the diagnostic and therapeutic algorithm: group A comprising children aged 2-14 years (n = 12) and group B comprising adolescents aged 15-18 years (n = 12). Patient characteristics, diagnosis and therapy-associated data, complications and clinical outcome were analysed. In both groups we found fractures in most of our patients (n = 19) followed by contusion of the soft tissues (n = 3). In group A most of our patients were injured as pedestrians in car accidents (n = 5) followed by low-energy blunt trauma (n = 3). The most common region of injury and traumatic ACS was the lower leg (n = 7) followed by the feet (n = 3). For fracture stabilisation most of the patients (n = 6) received an external fixator. The mean time from admission to the fasciotomy was 27.9 hours. In four patients a compartment pressure measurement was performed with pressure levels from 30 to 75 mmHg. A histological examination of soft tissue was performed in five patients. From fasciotomy to definitive wound closure 2.4 operations were necessary. The mean hospital stay was 18.9 days. In group B most of our patients had a motorcycle accident (n = 5). The most common region for traumatic ACS in this group was also the lower leg (n = 9). In most of the patients (n = 6) intramedullary nails could be implanted. The mean time from admission to the fasciotomy was 27.1 hours. In six patients a compartment pressure measurement was performed with pressures from 25 to 90 mmHg. In five patients a histological examination was performed. From fasciotomy to definitive wound closure 2.3 operations were necessary. The mean hospital stay was 18.4 days. Secondary fasciotomy closure was performed in all cases. A split-skin graft was only necessary in three patients (13%). We avoided primary closure in the same setting when the fasciotomy was performed. Thus, we found no difference between the two groups in the diagnostic procedures, the indication for fasciotomy, the number of operations needed from fasciotomy to definitive wound closure, time of hospitalisation and clinical outcome. The rate of permanent complications was 4.2% (one patient from group A), which means that nearly all patients experienced full recovery after fasciotomy. ACS represents a surgical emergency and the indication should be determined early even in doubtful cases to avoid complications.
Figures
References
-
- Volkmann R. Die ischaemischen Muskellähmungen und Kontrakturen. Centralbl Chir. 1881;8:801–803.
-
- Petersen F. Ueber ischämische Muskellähmung. Arch Klin Chir. 1888;37:675–677.
-
- Elliott KG, Johnstone AJ. Diagnosing acute compartment syndrome. J Bone Joint Surg Br. 2003;85:625–632. - PubMed
-
- Martin JT. Compartment syndromes: concepts and perspectives for the anesthesiologist. Anesth Analg. 1992;75:275–283. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
