

Universal methicillin-resistant Staphylococcus aureus (MRSA) surveillance for adults at hospital admission: an economic model and analysis
- PMID: 20402588
- PMCID: PMC3385994
- DOI: 10.1086/652524
Universal methicillin-resistant Staphylococcus aureus (MRSA) surveillance for adults at hospital admission: an economic model and analysis
Abstract
Background: Methicillin-resistant Staphylococcus aureus (MRSA) transmission and infections are a continuing problem in hospitals. Although some have recommended universal surveillance for MRSA at hospital admission to identify and to isolate MRSA-colonized patients, there is a need for formal economic studies to determine the cost-effectiveness of such a strategy.
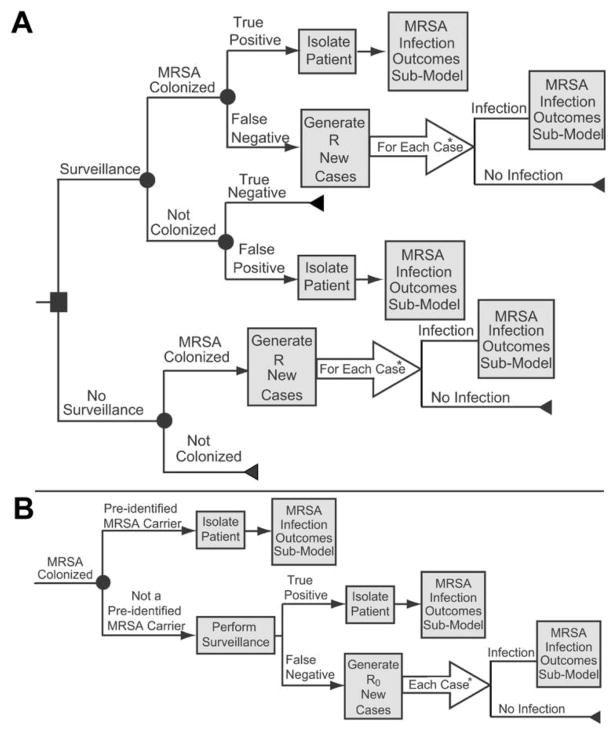
Methods: We developed a stochastic computer simulation model to determine the potential economic impact of performing MRSA surveillance (ie, single culture of an anterior nares specimen) for all hospital admissions at different MRSA prevalences and basic reproductive rate thresholds from the societal and third party-payor perspectives. Patients with positive surveillance culture results were placed under isolation precautions to prevent transmission by way of respiratory droplets. MRSA-colonized patients who were not isolated could transmit MRSA to other hospital patients.
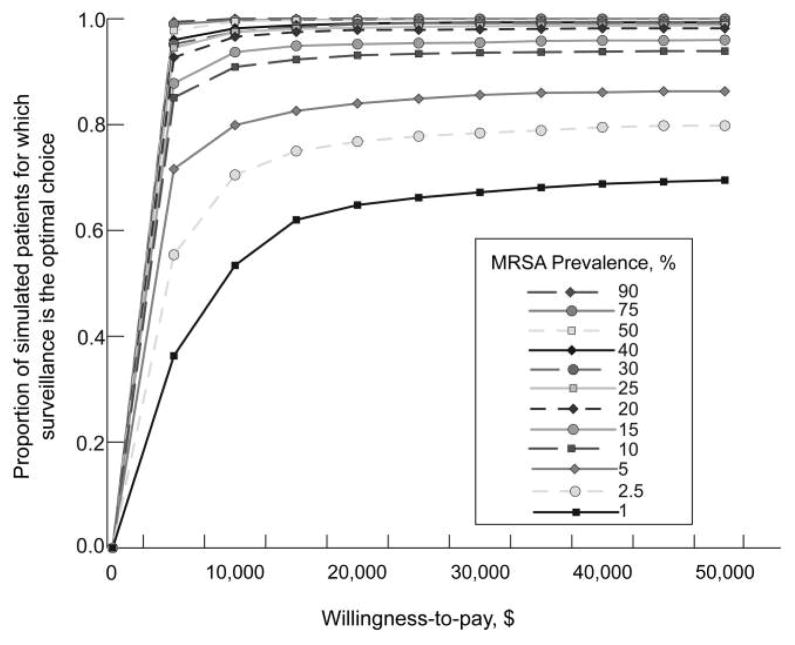
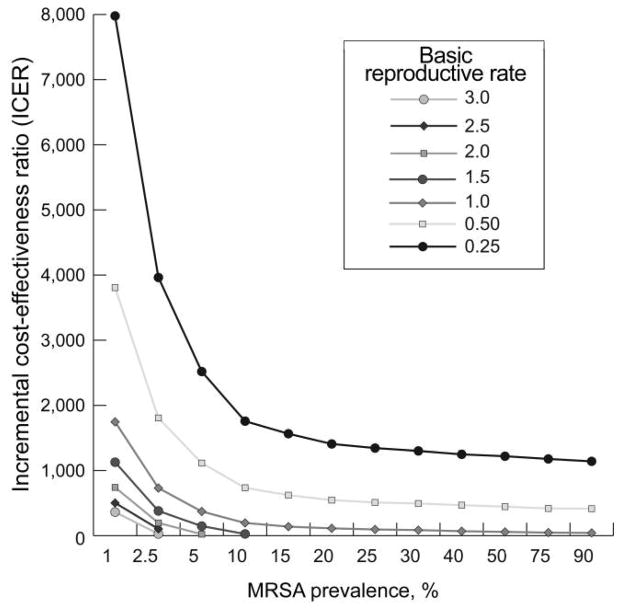
Results: The performance of universal MRSA surveillance was cost-effective (defined as an incremental cost-effectiveness ratio of less than $50,000 per quality-adjusted life-year) when the basic reproductive rate was 0.25 or greater and the prevalence was 1% or greater. In fact, surveillance was the dominant strategy when the basic reproductive rate was 1.5 or greater and the prevalence was 15% or greater, the basic reproductive rate was 2.0 or greater and the prevalence was 10% or greater, and the basic reproductive rate was 2.5 or greater and the prevalence was 5% or greater.
Conclusions: Universal MRSA surveillance of adults at hospital admission appears to be cost-effective at a wide range of prevalence and basic reproductive rate values. Individual hospitals and healthcare systems could compare their prevailing conditions (eg, the prevalence of MRSA colonization and MRSA transmission dynamics) with the benchmarks in our model to help determine their optimal local strategies.
Conflict of interest statement
Figures
References
-
- Beretta AL, Trabasso P, Stucchi RB, Moretti ML. Use of molecular epidemiology to monitor the nosocomial dissemination of methicillin-resistant Staphylococcus aureus in a university hospital from 1991 to 2001. Braz J Med Biol Res. 2004;37(9):1345–1351. - PubMed
-
- Harbarth S, Sax H, Fankhauser-Rodriguez C, Schrenzel J, Agostinho A, Pittet D. Evaluating the probability of previously unknown carriage of MRSA at hospital admission. Am J Med. 2006;119(3):275.e15–275.e23. - PubMed
-
- Farr BM. What to think if the results of the National Institutes of Health randomized trial of methicillin-resistant Staphylococcus aureus and van-comycin-resistant Enterococcus control measures are negative (and other advice to young epidemiologists): a review and an au revoir. Infect Control Hosp Epidemiol. 2006;27(10):1096–1106. - PubMed
-
- Wernitz MH, Swidsinski S, Weist K, et al. Effectiveness of a hospital-wide selective screening programme for methicillin-resistant Staphylococcus aureus (MRSA) carriers at hospital admission to prevent hospital-acquired MRSA infections. Clin Microbiol Infect. 2005;11(6):457–465. - PubMed
-
- Hsu CC, Lin YE, Chen YS, Liu YC, Muder RR. Validation study of artificial neural network models for prediction of methicillin-resistant Staphylococcus aureus carriage. Infect Control Hosp Epidemiol. 2008;29(7):607–614. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical