

Abuse liability of intravenous buprenorphine/naloxone and buprenorphine alone in buprenorphine-maintained intravenous heroin abusers
- PMID: 20403021
- PMCID: PMC3489277
- DOI: 10.1111/j.1360-0443.2009.02843.x
Abuse liability of intravenous buprenorphine/naloxone and buprenorphine alone in buprenorphine-maintained intravenous heroin abusers
Erratum in
- Addiction. 2010 Jul;105(7):1332
Abstract
Background: Sublingual buprenorphine is an effective maintenance treatment for opioid dependence, yet intravenous buprenorphine misuse occurs. A buprenorphine/naloxone formulation was developed to mitigate this misuse risk. This randomized, double-blind, cross-over study was conducted to assess the intravenous abuse potential of buprenorphine/naloxone compared with buprenorphine in buprenorphine-maintained injection drug users (IDUs).
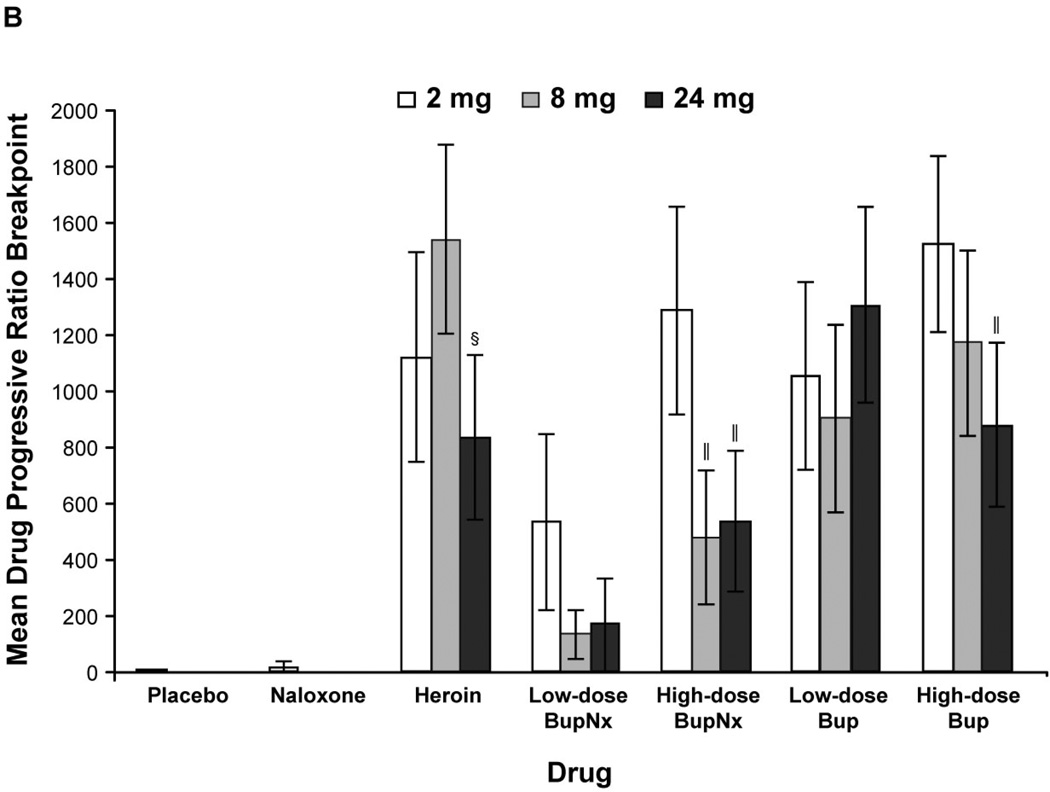
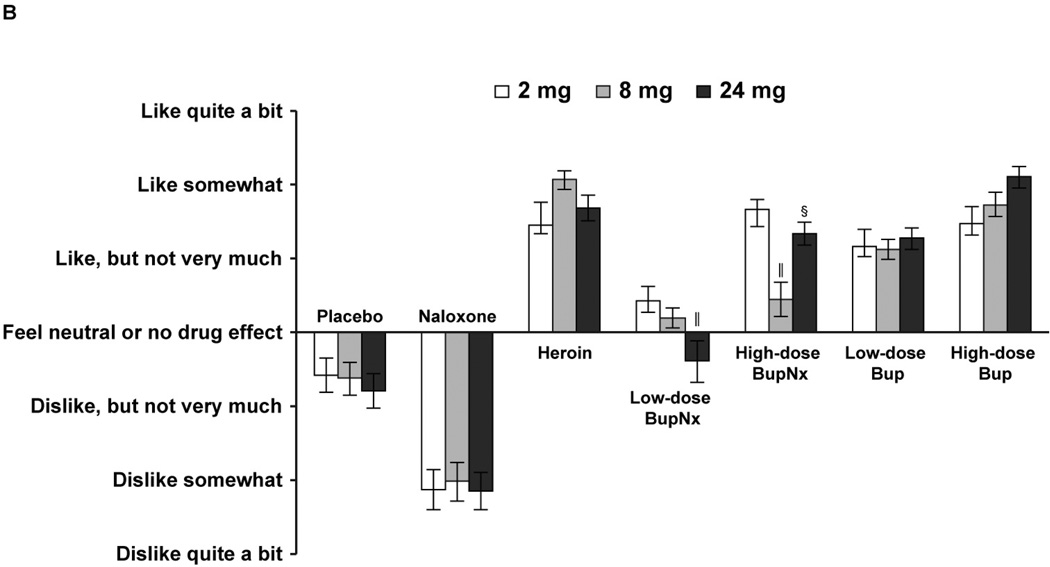
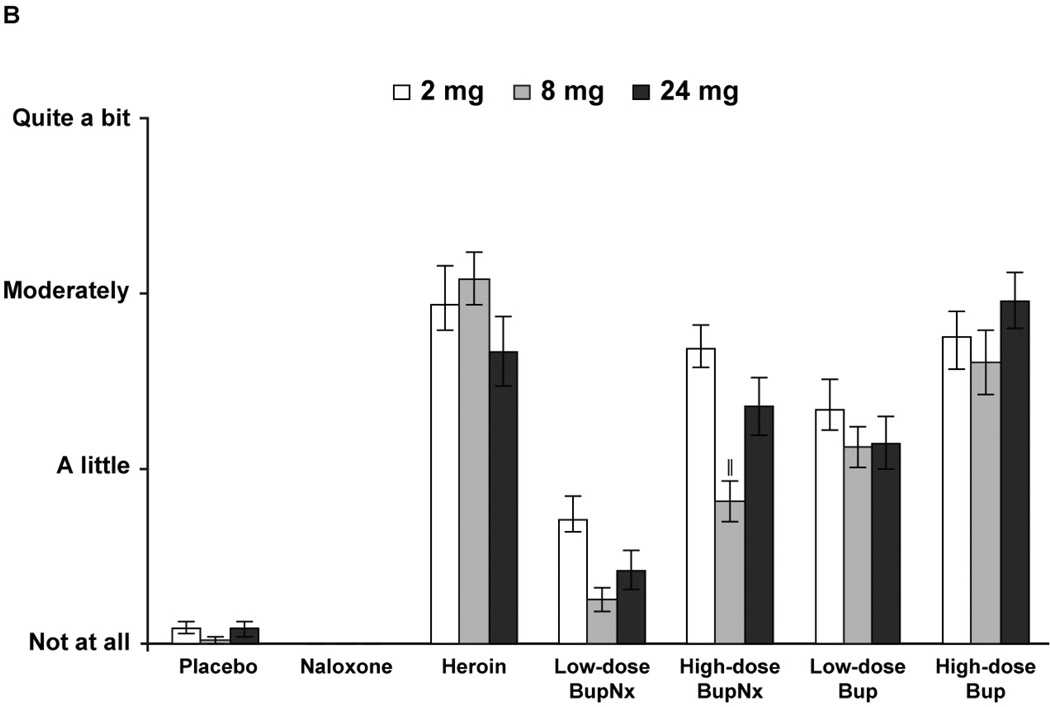
Methods: Intravenous heroin users (n = 12) lived in the hospital for 8-9 weeks and were maintained on each of three different sublingual buprenorphine doses (2 mg, 8 mg, 24 mg). Under each maintenance dose, participants completed laboratory sessions during which the reinforcing and subjective effects of intravenous placebo, naloxone, heroin and low and high doses of buprenorphine and buprenorphine/naloxone were examined. Every participant received each test dose under the three buprenorphine maintenance dose conditions.
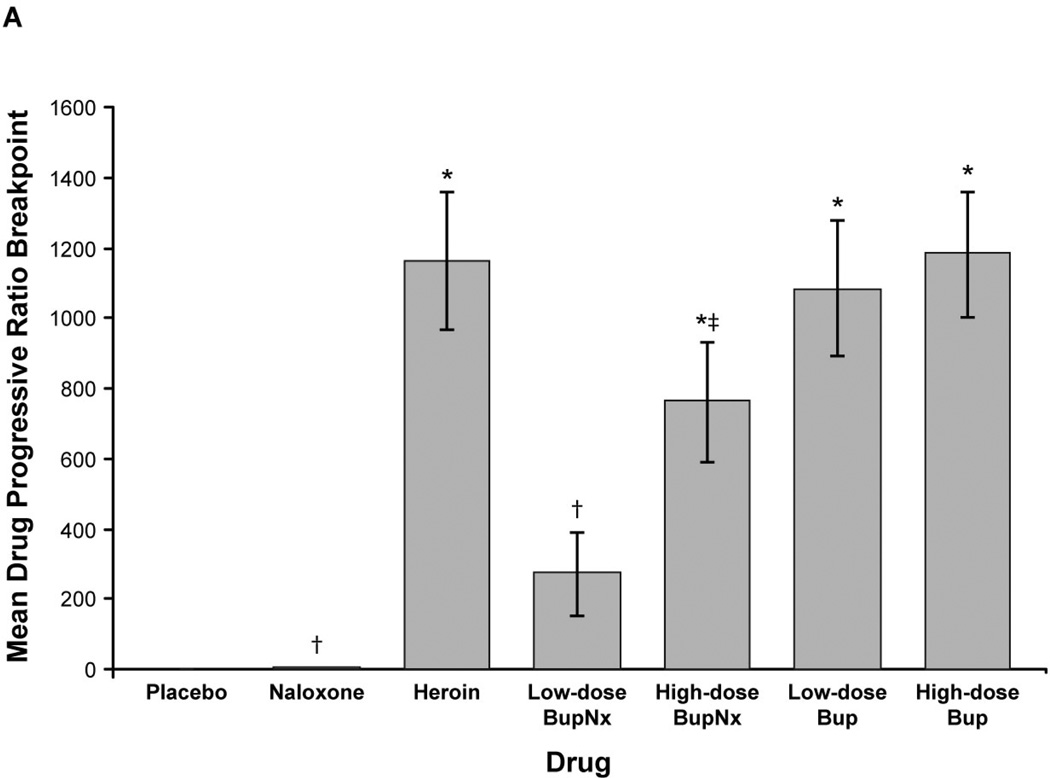
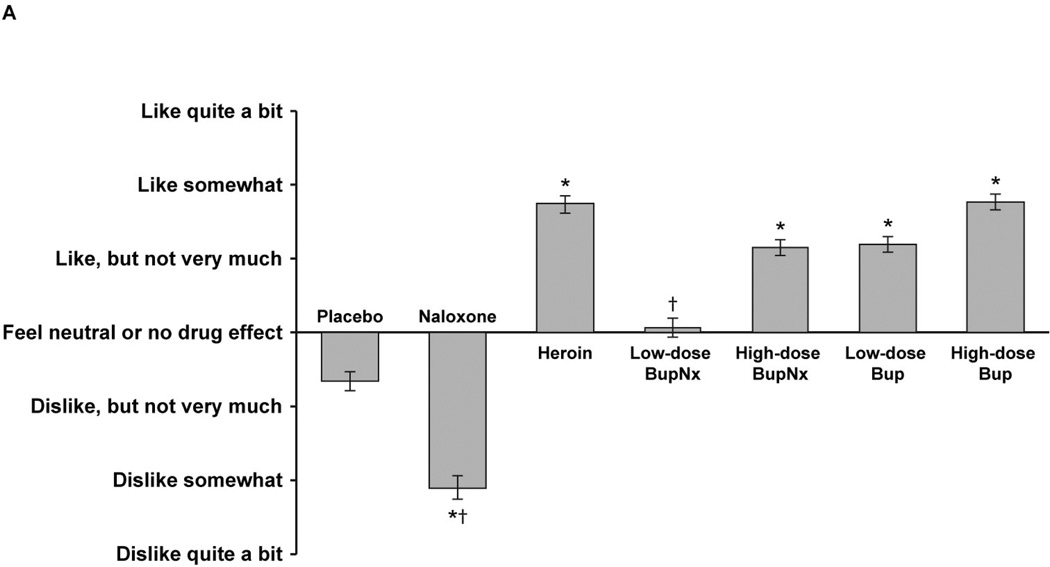
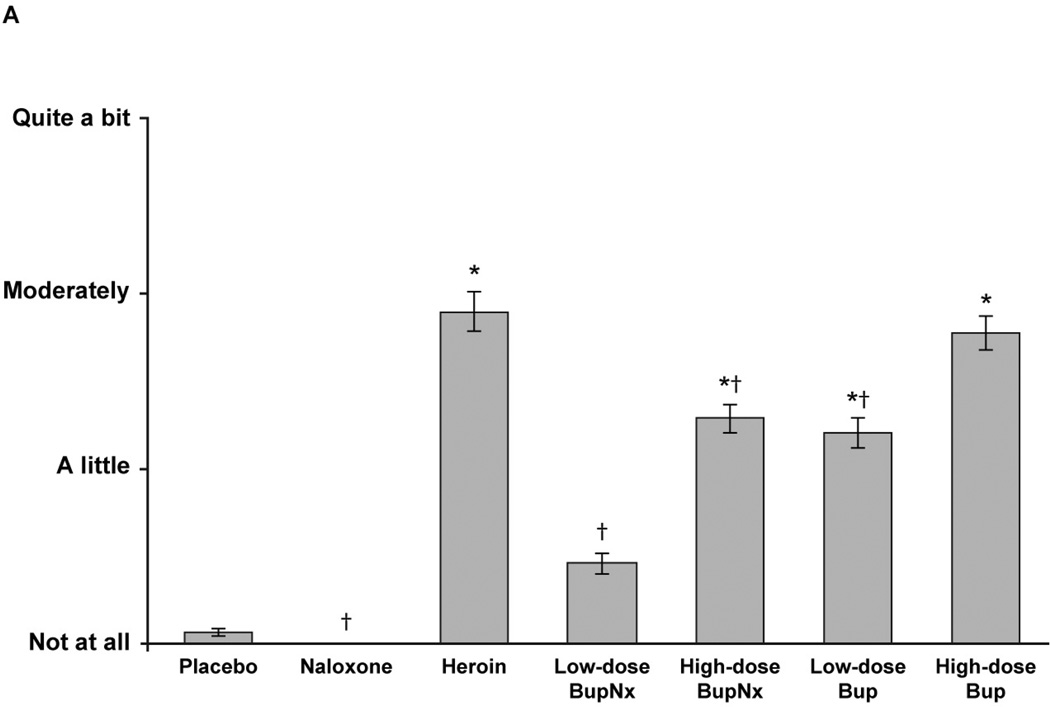
Results: Intravenous buprenorphine/naloxone was self-administered less frequently than buprenorphine or heroin (P < 0.0005). Participants were most likely to self-administer drug intravenously when maintained on the lowest sublingual buprenorphine dose. Subjective ratings of 'drug liking' and 'desire to take the drug again' were lower for buprenorphine/naloxone than for buprenorphine or heroin (P = 0.0001). Participants reported that they would pay significantly less money for buprenorphine/naloxone than for buprenorphine or heroin (P < 0.05). Seven adverse events were reported; most were mild and transient.
Conclusions: These data suggest that although the buprenorphine/naloxone combination has intravenous abuse potential, that potential is lower than it is for buprenorphine alone, particularly when participants received higher maintenance doses and lower buprenorphine/naloxone challenge doses. Buprenorphine/naloxone may be a reasonable option for managing the risk for buprenorphine misuse during opioid dependence treatment.
Trial registration: ClinicalTrials.gov NCT00710385.
Conflict of interest statement
The other authors have no conflicts to declare.
Figures
Similar articles
-
Abuse potential of intranasal buprenorphine versus buprenorphine/naloxone in buprenorphine-maintained heroin users.Addict Biol. 2015 Jul;20(4):784-98. doi: 10.1111/adb.12163. Epub 2014 Jul 25. Addict Biol. 2015. PMID: 25060839 Free PMC article. Clinical Trial.
-
Safety and tolerability of the switch from buprenorphine to buprenorphine/naloxone in an Italian addiction treatment centre.Clin Drug Investig. 2010;30 Suppl 1:27-31. doi: 10.2165/11536030-000000000-00000. Clin Drug Investig. 2010. PMID: 20450243
-
A prospective, randomized, multicenter acceptability and safety study of direct buprenorphine/naloxone induction in heroin-dependent individuals.Addiction. 2012 Jan;107(1):142-51. doi: 10.1111/j.1360-0443.2011.03577.x. Epub 2011 Oct 12. Addiction. 2012. PMID: 21749526 Clinical Trial.
-
Buprenorphine and naloxone for heroin dependence.Curr Psychiatry Rep. 2000 Dec;2(6):519-26. doi: 10.1007/s11920-000-0012-8. Curr Psychiatry Rep. 2000. PMID: 11123005 Review.
-
The clinical efficacy and abuse potential of combination buprenorphine-naloxone in the treatment of opioid dependence.Expert Opin Pharmacother. 2009 Oct;10(15):2537-44. doi: 10.1517/14656560903213405. Expert Opin Pharmacother. 2009. PMID: 19708849 Review.
Cited by
-
Buprenorphine treatment for narcotic addiction: not without risks.Innov Clin Neurosci. 2015 Mar-Apr;12(3-4):32-6. Innov Clin Neurosci. 2015. PMID: 25973324 Free PMC article.
-
MySafeRx: a mobile technology platform integrating motivational coaching, adherence monitoring, and electronic pill dispensing for enhancing buprenorphine/naloxone adherence during opioid use disorder treatment: a pilot study.Addict Sci Clin Pract. 2018 Sep 24;13(1):21. doi: 10.1186/s13722-018-0122-4. Addict Sci Clin Pract. 2018. PMID: 30249279 Free PMC article. Clinical Trial.
-
The reinforcing and subjective effects of intravenous and intranasal buprenorphine in heroin users.Pharmacol Biochem Behav. 2014 Jul;122:299-306. doi: 10.1016/j.pbb.2014.04.012. Epub 2014 May 2. Pharmacol Biochem Behav. 2014. PMID: 24793093 Free PMC article. Clinical Trial.
-
Inflammatory Pain Promotes Increased Opioid Self-Administration: Role of Dysregulated Ventral Tegmental Area μ Opioid Receptors.J Neurosci. 2015 Sep 2;35(35):12217-31. doi: 10.1523/JNEUROSCI.1053-15.2015. J Neurosci. 2015. PMID: 26338332 Free PMC article.
-
The pharmacodynamic and pharmacokinetic profile of intranasal crushed buprenorphine and buprenorphine/naloxone tablets in opioid abusers.Addiction. 2011 Aug;106(8):1460-73. doi: 10.1111/j.1360-0443.2011.03424.x. Epub 2011 May 3. Addiction. 2011. PMID: 21395892 Free PMC article. Clinical Trial.
References
-
- Carrieri MP, Amass L, Lucas GM, Vlahov D, Wodak A, Woody GE. Buprenorphine use: the international experience. Clin Infect Dis. 2006;43:S197–S215. - PubMed
-
- Teesson M, Mills K, Ross J, Darke S, Williamson A, Havard A. The impact of treatment on 3 years' outcome for heroin dependence: findings from the Australian Treatment Outcome Study (ATOS) Addiction. 2008;103:80–88. - PubMed
-
- Mathers BM, Degenhardt L, Phillips B, et al. Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review. Lancet. 2008;372:1733–1745. - PubMed
-
- Gossop M, Marsden J, Stewart D, Treacy S. Reduced injection risk and sexual risk behaviours after drug misuse treatment: results from the National Treatment Outcome Research Study. AIDS Care. 2002;14:77–93. - PubMed
-
- Gossop M, Marsden J, Stewart D, Kidd T. The National Treatment Outcome Research Study (NTORS): 4–5 year follow-up results. Addiction. 2003;98:291–303. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
