

Positive end-expiratory pressure may alter breathing cardiovascular variability and baroreflex gain in mechanically ventilated patients
- PMID: 20403192
- PMCID: PMC2868796
- DOI: 10.1186/1465-9921-11-38
Positive end-expiratory pressure may alter breathing cardiovascular variability and baroreflex gain in mechanically ventilated patients
Abstract
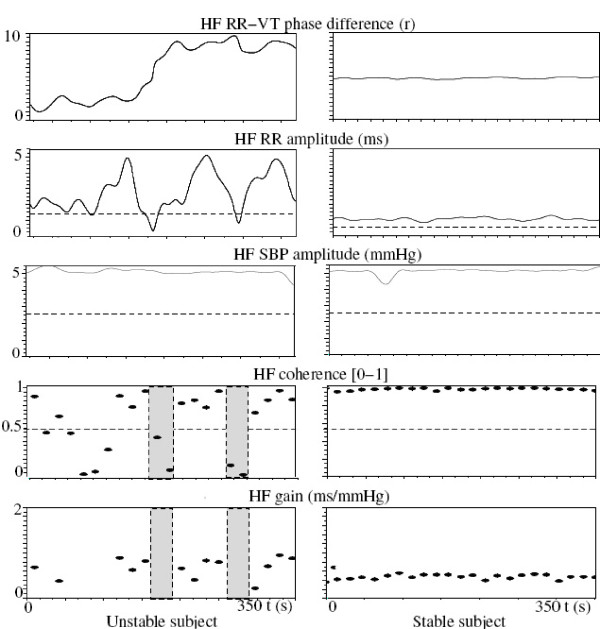
Background: Baroreflex allows to reduce sudden rises or falls of arterial pressure through parallel RR interval fluctuations induced by autonomic nervous system. During spontaneous breathing, the application of positive end-expiratory pressure (PEEP) may affect the autonomic nervous system, as suggested by changes in baroreflex efficiency and RR variability. During mechanical ventilation, some patients have stable cardiorespiratory phase difference and high-frequency amplitude of RR variability (HF-RR amplitude) over time and others do not. Our first hypothesis was that a steady pattern could be associated with reduced baroreflex sensitivity and HF-RR amplitude, reflecting a blunted autonomic nervous function. Our second hypothesis was that PEEP, widely used in critical care patients, could affect their autonomic function, promoting both steady pattern and reduced baroreflex sensitivity.
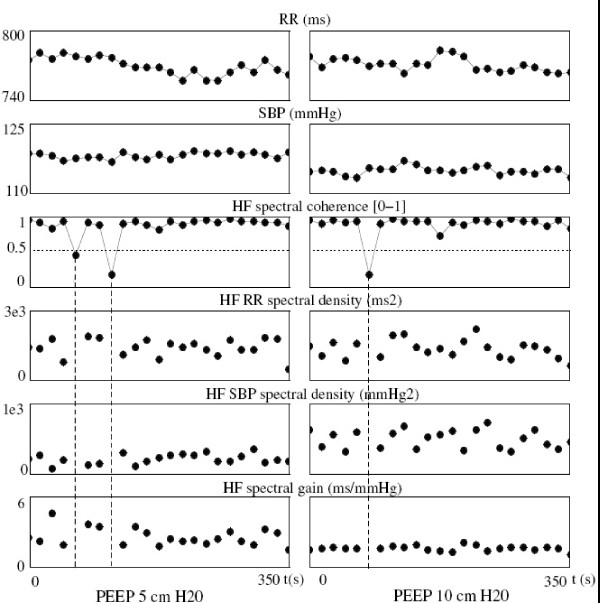
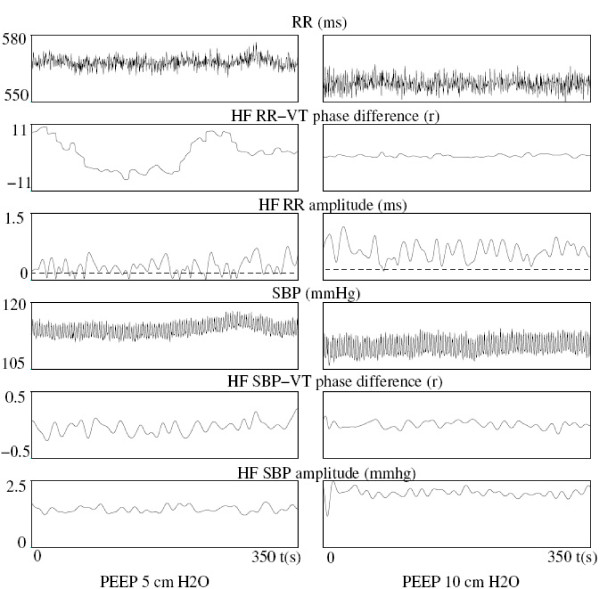
Methods: We tested the effect of increasing PEEP from 5 to 10 cm H2O on the breathing variability of arterial pressure and RR intervals, and on the baroreflex. Invasive arterial pressure, ECG and ventilatory flow were recorded in 23 mechanically ventilated patients during 15 minutes for both PEEP levels. HF amplitude of RR and systolic blood pressure (SBP) time series and HF phase differences between RR, SBP and ventilatory signals were continuously computed by complex demodulation. Cross-spectral analysis was used to assess the coherence and gain functions between RR and SBP, yielding baroreflex-sensitivity indices.
Results: At PEEP 10, the 12 patients with a stable pattern had lower baroreflex gain and HF-RR amplitude of variability than the 11 other patients. Increasing PEEP was generally associated with a decreased baroreflex gain and a greater stability of HF-RR amplitude and cardiorespiratory phase difference. Four patients who exhibited a variable pattern at PEEP 5 became stable at PEEP 10. At PEEP 10, a stable pattern was associated with higher organ failure score and catecholamine dosage.
Conclusions: During mechanical ventilation, stable HF-RR amplitude and cardiorespiratory phase difference over time reflect a blunted autonomic nervous function which might worsen as PEEP increases.
Figures
Similar articles
-
Breathing cardiovascular variability and baroreflex in mechanically ventilated patients.Am J Physiol Regul Integr Comp Physiol. 2008 Dec;295(6):R1934-40. doi: 10.1152/ajpregu.90475.2008. Epub 2008 Oct 15. Am J Physiol Regul Integr Comp Physiol. 2008. PMID: 18922962
-
Modulations of human autonomic function induced by positive pressure-assisted breathing.Clin Physiol Funct Imaging. 2006 Jan;26(1):15-20. doi: 10.1111/j.1475-097X.2005.00645.x. Clin Physiol Funct Imaging. 2006. PMID: 16398665
-
The effects of metronome breathing on the variability of autonomic activity measurements.J Manipulative Physiol Ther. 2000 Nov-Dec;23(9):610-4. doi: 10.1067/mmt.2000.110944. J Manipulative Physiol Ther. 2000. PMID: 11145801
-
Positive end-expiratory pressure for preterm infants requiring conventional mechanical ventilation for respiratory distress syndrome or bronchopulmonary dysplasia.Cochrane Database Syst Rev. 2019 Feb 26;2(2):CD004500. doi: 10.1002/14651858.CD004500.pub3. Cochrane Database Syst Rev. 2019. PMID: 30820939 Free PMC article.
-
Measurement of air trapping, intrinsic positive end-expiratory pressure, and dynamic hyperinflation in mechanically ventilated patients.Respir Care. 2005 Jan;50(1):110-23; discussion 123-4. Respir Care. 2005. PMID: 15636649 Review.
Cited by
-
Cardiac arrhythmias associated with volume-assured pressure support mode in a patient with autonomic dysfunction and mitochondrial disease.J Clin Sleep Med. 2021 Apr 1;17(4):853-857. doi: 10.5664/jcsm.9024. J Clin Sleep Med. 2021. PMID: 33231166 Free PMC article.
-
High-frequency power of heart rate variability can predict the outcome of thoracic surgical patients with acute respiratory distress syndrome on admission to the intensive care unit: a prospective, single-centric, case-controlled study.BMC Anesthesiol. 2018 Apr 2;18(1):34. doi: 10.1186/s12871-018-0497-5. BMC Anesthesiol. 2018. PMID: 29609546 Free PMC article.
References
-
- Annane D, Trabold F, Sharshar T, Jarrin I, Blanc AS, Raphael JC, Gajdos P. Inappropriate sympathetic activation at onset of septic shock; a spectral analysis approach. Am J Respir Crit Care Med. 1999;160:458–465. - PubMed
-
- Morris JA, Norris PR, Ozdas A, Waitman LR, Harrell FE Jr, Williams AE, Cao H, Jenkins JM. Reduced heart rate variability: an indicator of cardiac uncoupling and diminished physiologic reserve in 1425 trauma patients. J Trauma. 2006;60:1165–1174. doi: 10.1097/01.ta.0000220384.04978.3b. - DOI - PubMed
-
- Papaioannou VE, Maglaveras N, Houvarda I, Antoniadou E, Vretzakis G. Investigation of altered heart rate variability, nonlinear properties of heart rate signals, and organ dysfunction longitudinally over time in intensive care unit patients. J Crit Care. 2006;21(1):95–103. doi: 10.1016/j.jcrc.2005.12.007. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
