

Comparison of cardiovascular risk profiles among ethnic groups using population health surveys between 1996 and 2007
- PMID: 20403888
- PMCID: PMC2871219
- DOI: 10.1503/cmaj.091676
Comparison of cardiovascular risk profiles among ethnic groups using population health surveys between 1996 and 2007
Abstract
Background: Although people of South Asian, Chinese and black ethnic backgrounds represent about 60% of the world's population, most knowledge of cardiovascular risk is derived from studies conducted in white populations. We conducted a large, population-based comparison of cardiovascular risk among people of white, South Asian, Chinese and black ethnicity living in Ontario, Canada.
Methods: We examined the age- and sex-standardized prevalence of eight cardiovascular risk factors, heart disease and stroke among 154,653 white people, 3364 South Asian people, 3038 Chinese people and 2742 black people. For this study, we pooled respondent data from five cross-sectional health surveys conducted between 1996 and 2007: the National Population Health Survey of 1996 and the Canadian Community Health Survey, versions 1.1, 2.1, 3.1 and 4.1.
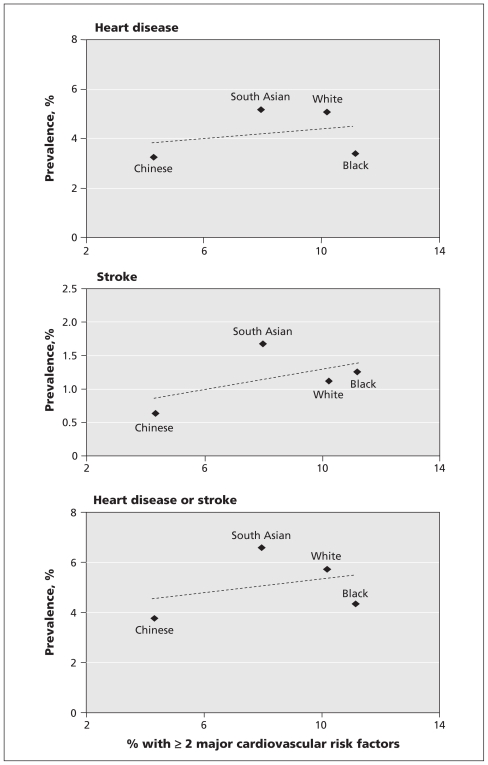
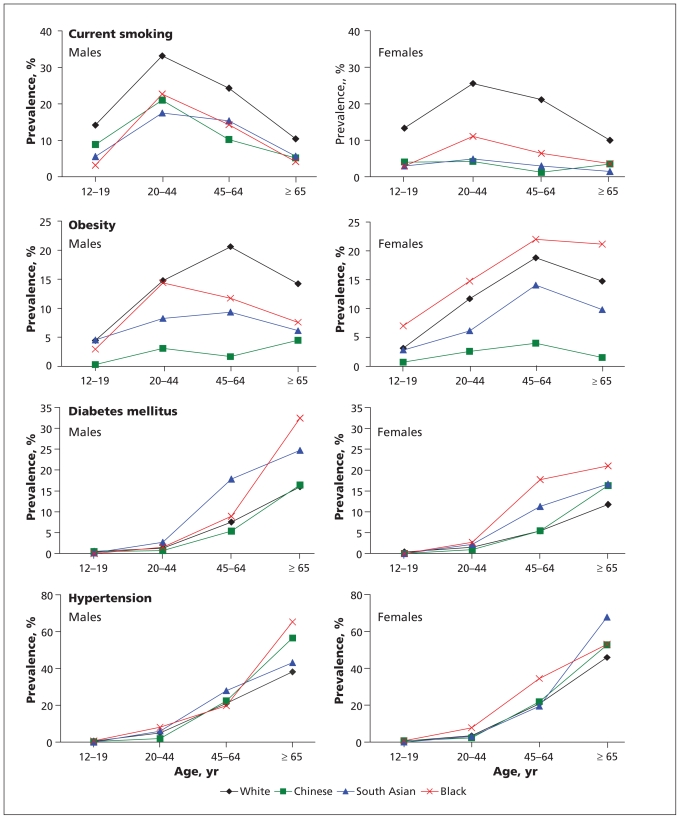
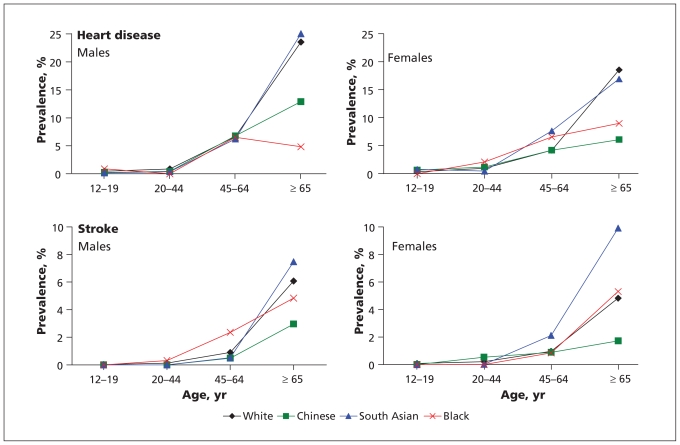
Results: The four ethnic groups varied considerably in the prevalence of the four major cardiovascular risk factors that we examined: for smoking, South Asian 8.6%, Chinese 8.7%, black 11.4% and white 24.8%; for obesity, Chinese 2.5%, South Asian 8.1%, black 14.1% and white 14.8%; for diabetes mellitus, white 4.2%, Chinese 4.3%, South Asian 8.1% and black 8.5%; and for hypertension, white 13.7%, Chinese 15.1%, South Asian 17.0% and black 19.8%. The prevalence of heart disease ranged from a low of 3.2% in the Chinese population to a high of 5.2% in the South Asian population, and the prevalence of stroke ranged from a low of 0.6% in the Chinese population to a high of 1.7% in the South Asian population. Although the black population had the least favourable cardiovascular risk factor profile overall, this group had a relatively low prevalence of heart disease (3.4%).
Interpretation: Ethnic groups living in Ontario had striking differences in cardiovascular risk profiles. Awareness of these differences may help in identifying priorities for the development of cardiovascular disease prevention programs for specific ethnic groups.
Figures
Comment in
-
Cardiovascular disease among South Asians.CMAJ. 2010 Sep 7;182(12):1334; author reply 1334. doi: 10.1503/cmaj.110-2097. CMAJ. 2010. PMID: 20823191 Free PMC article. No abstract available.
References
-
- Murray CJ, Lopez AD. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet. 1997;349:1269–76. - PubMed
-
- Yusuf S, Reddy S, Ounpuu S, et al. Global burden of cardiovascular diseases: part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation. 2001;104:2746–53. - PubMed
-
- Anand SS, Yusuf S, Vuksan V, et al. Differences in risk factors, atherosclerosis, and cardiovascular disease between ethnic groups in Canada: the Study of Health Assessment and Risk in Ethnic groups (SHARE) Lancet. 2000;356:279–84. - PubMed
-
- Lip GY, Barnett AH, Bradbury A, et al. Ethnicity and cardiovascular disease prevention in the United Kingdom: a practical approach to management. J Hum Hypertens. 2007;21:183–211. - PubMed
-
- Mensah GA, Mokdad AH, Ford ES, et al. State of disparities in cardiovascular health in the United States. Circulation. 2005;111:1233–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical