

Clinical and imaging heterogeneity of polymicrogyria: a study of 328 patients
- PMID: 20403963
- PMCID: PMC2859156
- DOI: 10.1093/brain/awq078
Clinical and imaging heterogeneity of polymicrogyria: a study of 328 patients
Abstract
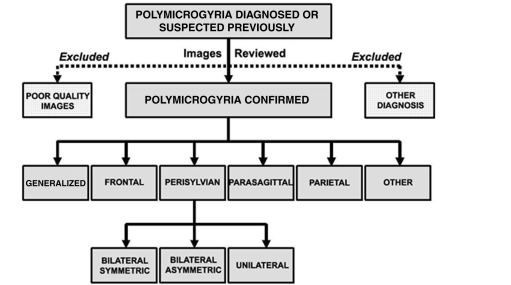
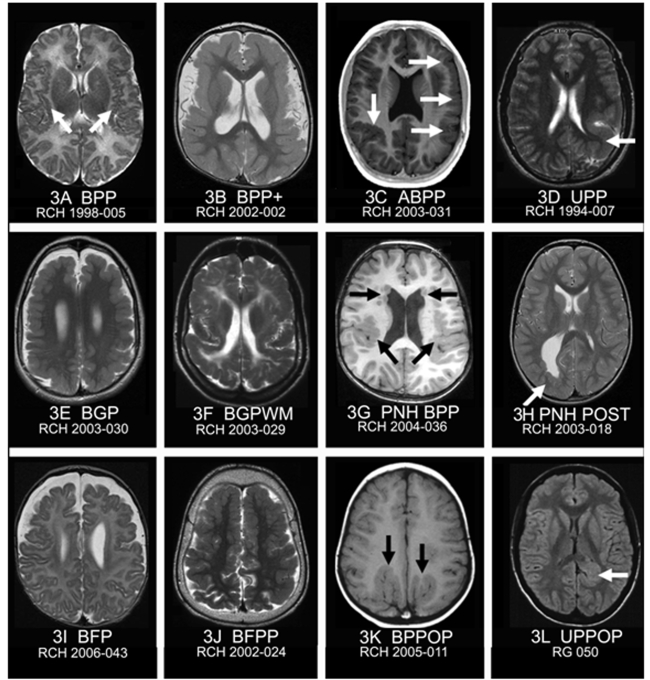
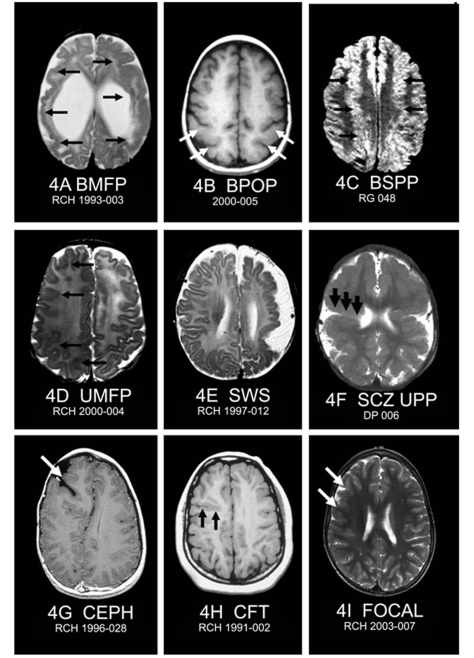
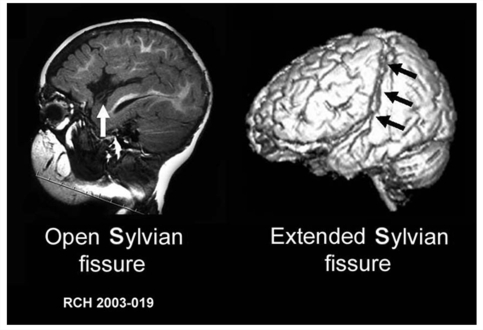
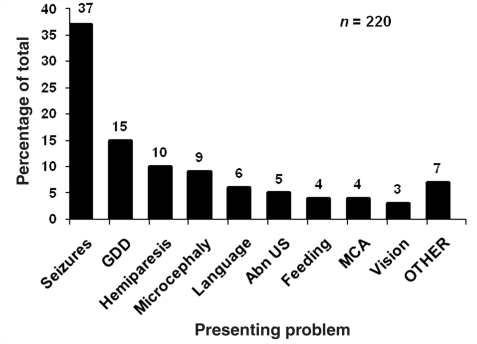
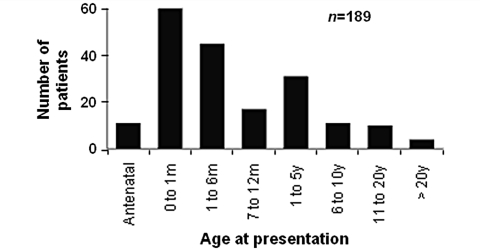
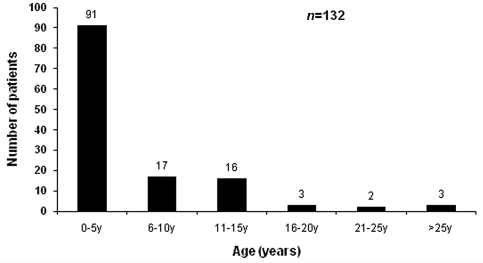
Polymicrogyria is one of the most common malformations of cortical development and is associated with a variety of clinical sequelae including epilepsy, intellectual disability, motor dysfunction and speech disturbance. It has heterogeneous clinical manifestations and imaging patterns, yet large cohort data defining the clinical and imaging spectrum and the relative frequencies of each subtype are lacking. The aims of this study were to determine the types and relative frequencies of different polymicrogyria patterns, define the spectrum of their clinical and imaging features and assess for clinical/imaging correlations. We studied the imaging features of 328 patients referred from six centres, with detailed clinical data available for 183 patients. The ascertainment base was wide, including referral from paediatricians, geneticists and neurologists. The main patterns of polymicrogyria were perisylvian (61%), generalized (13%), frontal (5%) and parasagittal parieto-occipital (3%), and in 11% there was associated periventricular grey matter heterotopia. Each of the above patterns was further divided into subtypes based on distinguishing imaging characteristics. The remaining 7% were comprised of a number of rare patterns, many not described previously. The most common clinical sequelae were epileptic seizures (78%), global developmental delay (70%), spasticity (51%) and microcephaly (50%). Many patients presented with neurological or developmental abnormalities prior to the onset of epilepsy. Patients with more extensive patterns of polymicrogyria presented at an earlier age and with more severe sequelae than those with restricted or unilateral forms. The median age at presentation for the entire cohort was 4 months with 38% presenting in either the antenatal or neonatal periods. There were no significant differences between the prevalence of epilepsy for each polymicrogyria pattern, however patients with generalized and bilateral forms had a lower age at seizure onset. There was significant skewing towards males with a ratio of 3:2. This study expands our understanding of the spectrum of clinical and imaging features of polymicrogyria. Progression from describing imaging patterns to defining anatomoclinical syndromes will improve the accuracy of prognostic counselling and will aid identification of the aetiologies of polymicrogyria, including genetic causes.
Figures
References
-
- Aicardi J. Aicardi syndrome. Brain Dev. 2005;27:164–71. - PubMed
-
- Barkovich AJ, Kuzniecky RI, Jackson GD, Guerrini R, Dobyns WB. A developmental and genetic classification for malformations of cortical development. Neurology. 2005;65:1873–87. - PubMed
-
- Chang BS, Piao X, Bodell A, Basel-Vanagaite L, Straussberg R, Dobyns WB, et al. Bilateral frontoparietal polymicrogyria: clinical and radiological features in 10 families with linkage to chromosome 16. Ann Neurol. 2003;53:596–606. - PubMed
-
- Chang BS, Piao X, Giannini C, Cascino GD, Scheffer I, Woods CG, et al. Bilateral generalized polymicrogyria (BGP): a distinct syndrome of cortical malformation. Neurology. 2004;62:1722–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
