

Gray and white matter water diffusion in the syndromic variants of frontotemporal dementia
- PMID: 20404309
- PMCID: PMC2860485
- DOI: 10.1212/WNL.0b013e3181d9edde
Gray and white matter water diffusion in the syndromic variants of frontotemporal dementia
Abstract
Objective: To use diffusion tensor imaging (DTI) to assess gray matter and white matter tract diffusion in behavioral variant frontotemporal dementia (bvFTD), semantic dementia (SMD), and progressive nonfluent aphasia (PNFA).
Methods: This was a case-control study where 16 subjects with bvFTD, 7 with PNFA, and 4 with SMD were identified and matched by age and gender to 19 controls. All subjects had 3-T head MRI with a DTI sequence with diffusion encoding in 21 directions. Gray matter mean diffusivity (MD) was assessed using a region-of-interest (ROI) and voxel-level approach, and voxel-based morphometry was used to assess patterns of gray matter loss. White matter tract diffusivity (fractional anisotropy and radial diffusivity) was assessed by placing ROIs on tracts of interest.
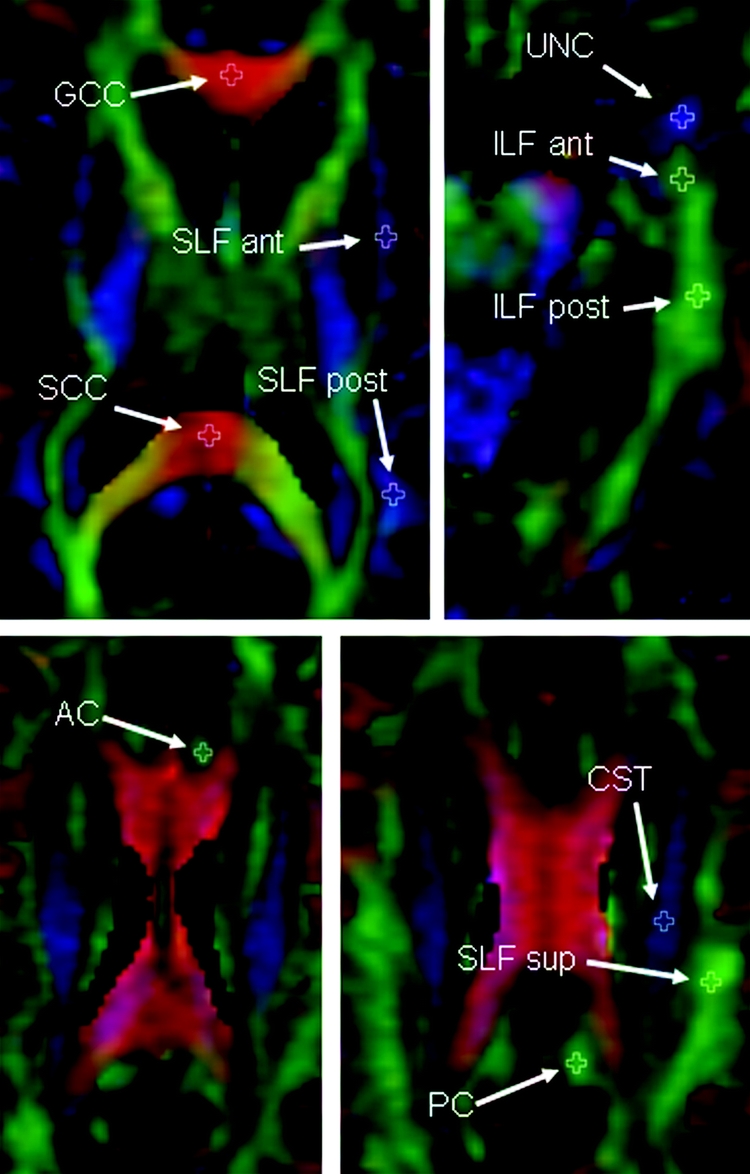
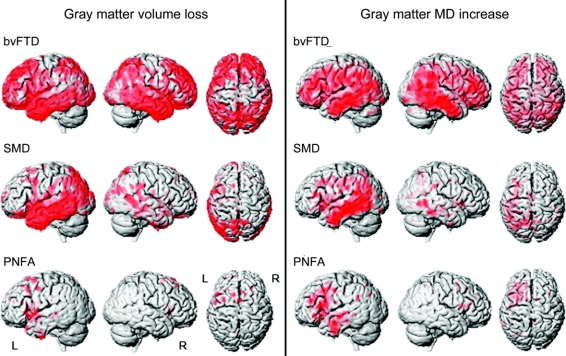
Results: In bvFTD, increased gray matter MD and gray matter loss were identified bilaterally throughout frontal and temporal lobes, with abnormal diffusivity observed in white matter tracts that connect to these regions. In SMD, gray matter loss and increased MD were identified predominantly in the left temporal lobe, with tract abnormalities observed in the inferior longitudinal fasciculus and uncinate fasciculus. In PNFA, gray matter loss and increased MD were observed in left inferior frontal lobe, insula, and supplemental motor area, with tract abnormalities observed in the superior longitudinal fasciculus.
Conclusions: The diffusivity of gray matter is increased in regions that are atrophic in frontotemporal dementia, suggesting disruption of the cytoarchitecture of remaining tissue. Furthermore, damage was identified in white matter tracts that interconnect these regions, supporting the hypothesis that these diseases involve different and specific brain networks.
Figures

Similar articles
-
Atrophy, hypometabolism and white matter abnormalities in semantic dementia tell a coherent story.Brain. 2011 Jul;134(Pt 7):2025-35. doi: 10.1093/brain/awr119. Epub 2011 Jun 6. Brain. 2011. PMID: 21646331
-
MRI signatures of brain macrostructural atrophy and microstructural degradation in frontotemporal lobar degeneration subtypes.J Alzheimers Dis. 2013;33(2):431-44. doi: 10.3233/JAD-2012-121156. J Alzheimers Dis. 2013. PMID: 22976075 Free PMC article. Clinical Trial.
-
White matter damage in frontotemporal lobar degeneration spectrum.Cereb Cortex. 2012 Dec;22(12):2705-14. doi: 10.1093/cercor/bhr288. Epub 2011 Oct 10. Cereb Cortex. 2012. PMID: 21988828
-
Diffusion tensor imaging in Alzheimer's disease and mild cognitive impairment.Behav Neurol. 2009;21(1):39-49. doi: 10.3233/BEN-2009-0234. Behav Neurol. 2009. PMID: 19847044 Free PMC article. Review.
-
Primary progressive aphasia and Alzheimer's disease: brief history, recent evidence.Curr Neurol Neurosci Rep. 2012 Dec;12(6):709-14. doi: 10.1007/s11910-012-0307-2. Curr Neurol Neurosci Rep. 2012. PMID: 22932755 Review.
Cited by
-
Patterns of brain atrophy in clinical variants of frontotemporal lobar degeneration.Dement Geriatr Cogn Disord. 2013;35(1-2):34-50. doi: 10.1159/000345523. Epub 2013 Jan 9. Dement Geriatr Cogn Disord. 2013. PMID: 23306166 Free PMC article.
-
Widespread structural and functional connectivity changes in amyotrophic lateral sclerosis: insights from advanced neuroimaging research.Neural Plast. 2012;2012:473538. doi: 10.1155/2012/473538. Epub 2012 Jun 10. Neural Plast. 2012. PMID: 22720174 Free PMC article. Review.
-
Structural and functional brain connectivity in presymptomatic familial frontotemporal dementia.Neurology. 2013 Feb 26;80(9):814-23. doi: 10.1212/WNL.0b013e31828407bc. Epub 2013 Feb 6. Neurology. 2013. PMID: 23390180 Free PMC article.
-
Neuroimaging biomarkers of neurodegenerative diseases and dementia.Semin Neurol. 2013 Sep;33(4):386-416. doi: 10.1055/s-0033-1359312. Epub 2013 Nov 14. Semin Neurol. 2013. PMID: 24234359 Free PMC article. Review.
-
Brain white matter shape changes in amyotrophic lateral sclerosis (ALS): a fractal dimension study.PLoS One. 2013 Sep 9;8(9):e73614. doi: 10.1371/journal.pone.0073614. eCollection 2013. PLoS One. 2013. PMID: 24040000 Free PMC article.
References
-
- Basser PJ, Mattiello J, LeBihan D. Estimation of the effective self-diffusion tensor from the NMR spin echo. J Magn Reson B 1994;103:247–254. - PubMed
-
- Grossman M, McMillan C, Moore P, et al. What's in a name: voxel-based morphometric analyses of MRI and naming difficulty in Alzheimer's disease, frontotemporal dementia and corticobasal degeneration. Brain 2004;127:628–649. - PubMed
Publication types
MeSH terms
Grants and funding
- P50 AG16574/AG/NIA NIH HHS/United States
- R01 HL70825/HL/NHLBI NIH HHS/United States
- R01-AG023195/AG/NIA NIH HHS/United States
- P50 AG016574/AG/NIA NIH HHS/United States
- R01-AG11378/AG/NIA NIH HHS/United States
- C06 RR018898/RR/NCRR NIH HHS/United States
- P50-AG16574/AG/NIA NIH HHS/United States
- P50 AG16574/P1/AG/NIA NIH HHS/United States
- R01 AG15866/AG/NIA NIH HHS/United States
- R01 EB00229/EB/NIBIB NIH HHS/United States
- U24 AG026395/AG/NIA NIH HHS/United States
- P50 NS40256/NS/NINDS NIH HHS/United States
- U01 AG 024904/AG/NIA NIH HHS/United States
- R01 MH79261/MH/NIMH NIH HHS/United States
- R01 AG11378/AG/NIA NIH HHS/United States
- U01 AG024904-01/AG/NIA NIH HHS/United States
- HD49078/HD/NICHD NIH HHS/United States
- U01 AG016976/AG/NIA NIH HHS/United States
- UL1 RR 24150/RR/NCRR NIH HHS/United States
- K23 AG030935/AG/NIA NIH HHS/United States
- U01 AG06786/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical