

doi: 10.4184/asj.2008.2.2.114.
Epub 2008 Dec 31.
Posterior surgery for cervical myelopathy: laminectomy, laminectomy with fusion, and laminoplasty
Affiliations
- PMID: 20404967
- PMCID: PMC2852088
- DOI: 10.4184/asj.2008.2.2.114
Item in Clipboard
Posterior surgery for cervical myelopathy: laminectomy, laminectomy with fusion, and laminoplasty
Asian Spine J.
2008 Dec.
No abstract available
Figures
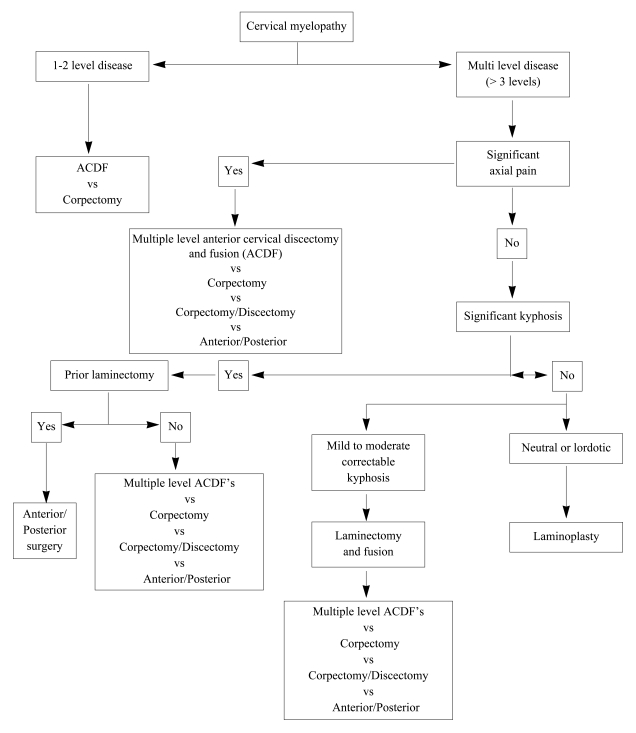
General guidelines for surgical management of cervical myelopathy
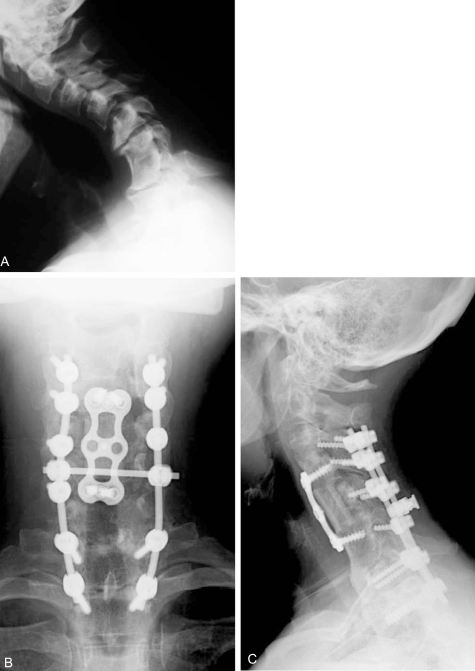
Fifty-two year old woman with post-laminectomy kyphosis and myelopathy. (A) Several factors contribute to her kyphosis: 1) an anterior cervical discectomy without fusion at C6-7 in the remote past that healed in kyphosis; 2) severe disc degeneration at C5-6 and C7-T1; 3) iatrogenic spondylolisthesis at C4-5; and 4) multilevel laminectomy. (B and C) AP and lateral xrays after C5 corpectomy, C3-4 ACDF, and posterior fusion performed to correct kyphosis and decompress the spinal canal.
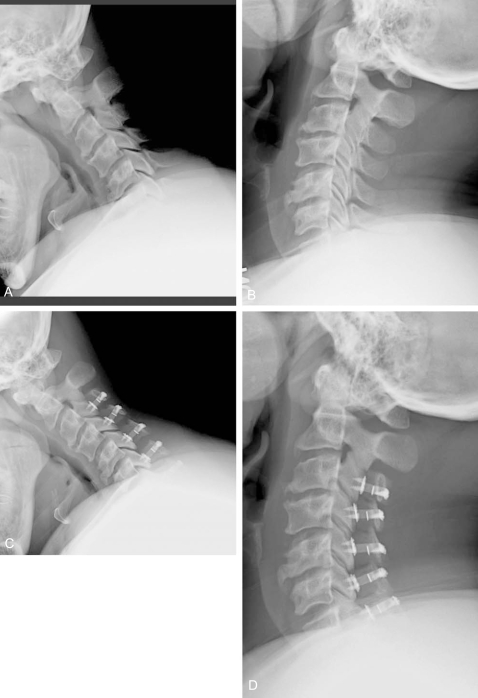
Laminoplasty is a relatively motion-preserving procedure. Flexion-extension xrays before (A and B) and at 3 months after (C and D) multilevel laminoplasty demonstrate preservation of range of motion. In many cases, however, some loss of motion occurs after laminoplasty.
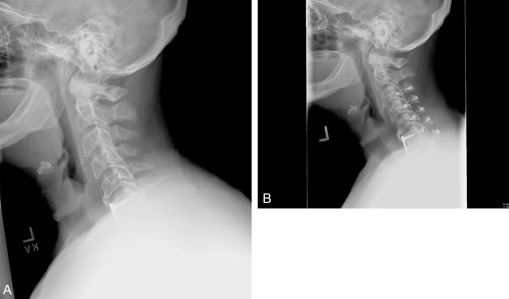
Even with laminoplasty, some loss of lordosis may occur. Note in this patient, a subtle loss of lordosis postoperatively (A) versus preoperatively (B).
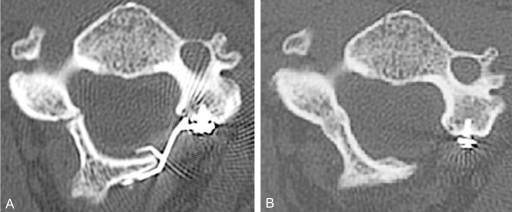
Axial CT scans of a plated laminoplasty. (A) At 3 months postoperatively, note that the hinge was inadvertently made too "floppy", with both the dorsal and ventral cortices being cracked. (B) At 2 year follow up, however, the hinge has completely healed and remodeled. Plates provide the most stable form of laminoplasty fixation and are particularly helpful in cases such as these with "floppy" hinges.

There are four elements of a properly positioned patient for posterior cervical surgery. 1) Tongs are used to suspend the eyes and face from pressure, 2) the bed is placed into reverse trendelenberg to decrease venous pooling at the surgical site, 3) longitudinal bolsters (not seen) running laterally along the thoracoabdominal regions also decrease abdominal pressure and thus the venous pressure head at the surgical site, and 4) the neck is placed into a neutral to slightly flexed posture in order to decrease inter-laminar "shingling" or overlap. If a fusion is performed, the neck should be placed into a more lordotic postion prior to locking down the instrumentation.
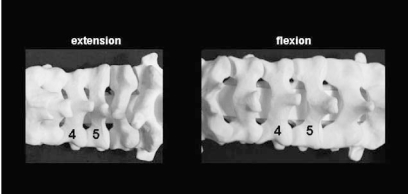
In extension (left), there is greater overlap or "shingling" of the adjacent laminae, making surgery more difficult to perform. In relative flexion (right), there is less overlap, but greater care must be taken during exposure to avoid plunging into the canal. A relatively flexed posture will also tend to increase spinal canal dimensions and thus be neurologically safer in those who have severe stenosis and worsening of neurologic symptoms in extension.
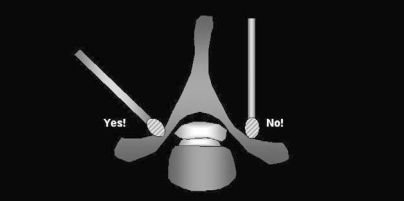
Burr orientation: When creating either the hinge or open sides, the burr should be placed at the lateral mass-laminar junction and then oriented perpendicular to the lamina (left). The burr should not be oriented perpendicular to the floor (right), as this will lead to unnecessary removal of facet and make it more difficult to achieve the goal of entering and decompressing the spinal canal.
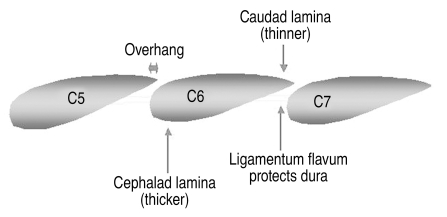
Laminar anatomy. A sagittal representation of the lateral mass-laminar junction, where both the hinge and open sides of the laminoplasty are created. Note that the cepahalad portion of the lamina is 1) thicker than the caudal end, 2) covered by an "overhang" from the lamina above (dependent in part on the amount of flexion during positioning), and 3) not protected on its ventral surface by ligamentum flavum. For these reasons, burring is more difficult on the cephalad versus caudad portion of the lamina. If the laminoplasty fails to open, inspect the cephalad portion of the lamina for inadequate thinning. Note also that relative flexion during positioning will decrease the amount of inter-laminar overhang, making surgery easier to perform.
References
-
- Geck MJ, Eismont FJ. Surgical options for the treatment of cervical spondylotic myelopathy. Orthop Clin North Am. 2002;33:329–348. - PubMed
-
- Hirabayashi K, Bohlman HH. Multilevel cervical spondylosis. Laminoplasty versus anterior decompression. Spine. 1995;20:1732–1734. - PubMed
-
- Mikawa Y, Shikata J, Yamamuro T. Spinal deformity and instability after multilevel cervical laminectomy. Spine. 1987;12:6–11. - PubMed
-
- Kato Y, Iwasaki M, Fuji T, Yonenobu K, Ochi T. Long-term follow-up results of laminectomy for cervical myelopathy caused by ossification of the posterior longitudinal ligament. J Neurosurg. 1998;89:217–223. - PubMed
-
- Matsunaga S, Sakou T, Nakanisi K. Analysis of the cervical spine alignment following laminoplasty and laminectomy. Spinal Cord. 1999;37:20–24. - PubMed
LinkOut - more resources
Full Text Sources
