

Tuberculous uveitis
- PMID: 20404986
- PMCID: PMC2855660
- DOI: 10.4103/0974-9233.58421
Tuberculous uveitis
Abstract
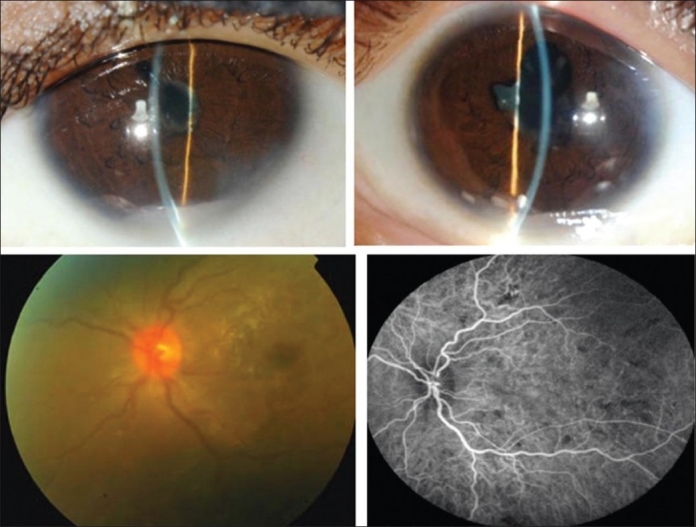
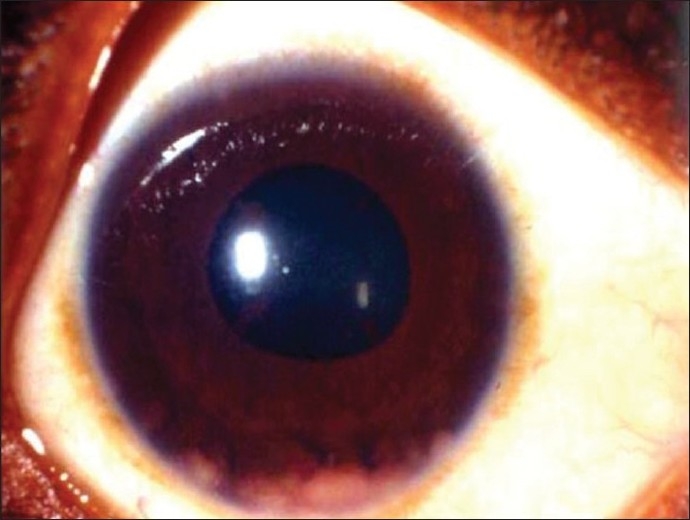
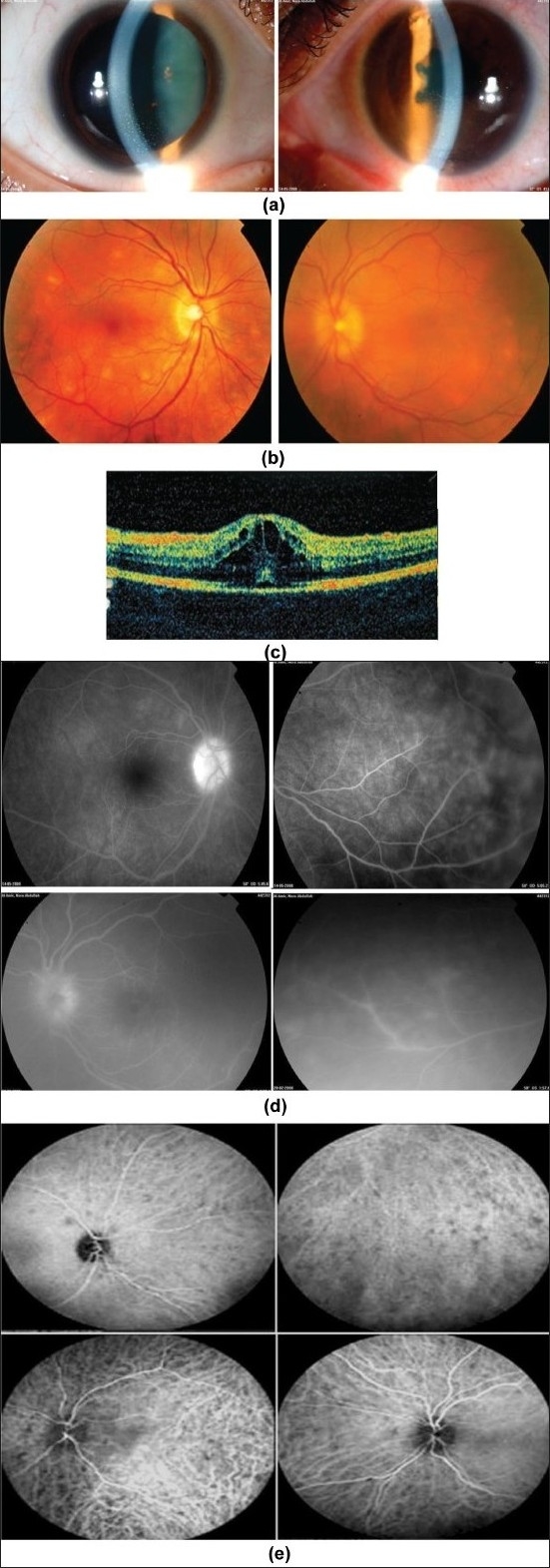
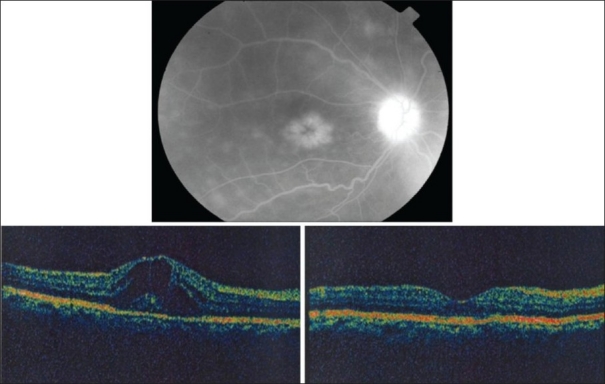
In recent years, ocular involvement due to TB has re-emerged. Tuberculous uveitis is a readily treatable disease and the consequences of delay in either ocular or systemic diagnosis can be very serious for the patient. It is important to have a high index of suspicion of the diagnosis in patients with unexplained chronic uveitis and this will be influenced by the socio-economic circumstances, family history, ethnic origin, and previous medical history of the patient. Treatment with antituberculous therapy combined with systemic corticosteroids resolves inflammation without recurrences after medical therapy.
Keywords: Diagnosis; Treatment; Tuberculosis Uveitis.
Conflict of interest statement
Figures
Similar articles
-
Tuberculous uveitis, a resurgent and underdiagnosed disease.Int Ophthalmol. 2009 Apr;29(2):67-74. doi: 10.1007/s10792-007-9071-8. Epub 2007 May 8. Int Ophthalmol. 2009. PMID: 17486298
-
Clinical and optical coherence tomographic findings and outcome of treatment in patients with presumed tuberculous uveitis.Int Ophthalmol. 2008 Dec;28(6):413-23. doi: 10.1007/s10792-007-9170-6. Epub 2007 Nov 22. Int Ophthalmol. 2008. PMID: 18034214
-
Ocular tuberculosis: current perspectives.Clin Ophthalmol. 2015 Nov 26;9:2223-7. doi: 10.2147/OPTH.S65254. eCollection 2015. Clin Ophthalmol. 2015. PMID: 26648690 Free PMC article. Review.
-
Diagnosis and treatment of tuberculous uveitis in a low endemic setting.Int J Infect Dis. 2013 Nov;17(11):e993-9. doi: 10.1016/j.ijid.2013.03.019. Epub 2013 May 22. Int J Infect Dis. 2013. PMID: 23706496
-
[Recent advances in tuberculous uveitis].Zhonghua Yan Ke Za Zhi. 2010 Sep;46(9):861-4. Zhonghua Yan Ke Za Zhi. 2010. PMID: 21092566 Review. Chinese.
Cited by
-
Primed Mycobacterial Uveitis (PMU) as a Model for Post-Infectious Uveitis.J Vis Exp. 2021 Dec 17;(178):10.3791/62925. doi: 10.3791/62925. J Vis Exp. 2021. PMID: 34978282 Free PMC article.
-
Prevalence of presumed ocular tuberculosis among pulmonary tuberculosis patients in a tertiary hospital in the Philippines.J Ophthalmic Inflamm Infect. 2013 Jan 3;3(1):1. doi: 10.1186/1869-5760-3-1. J Ophthalmic Inflamm Infect. 2013. PMID: 23514121 Free PMC article.
-
Types of Fundus Involvement in Intraocular Tuberculosis.Turk Thorac J. 2022 Sep;23(5):322-330. doi: 10.5152/TurkThoracJ.2022.21207. Turk Thorac J. 2022. PMID: 35943072 Free PMC article.
-
Pattern of uveitis at a referral center in Iraq.Middle East Afr J Ophthalmol. 2014 Oct-Dec;21(4):291-5. doi: 10.4103/0974-9233.142263. Middle East Afr J Ophthalmol. 2014. PMID: 25371632 Free PMC article.
-
Tuberculosis of the eye, case series study.J Med Life. 2022 Aug;15(8):1058-1062. doi: 10.25122/jml-2021-0343. J Med Life. 2022. PMID: 36188648 Free PMC article.
References
-
- Centers for Disease Control and Prevention. Case definitions for infectious conditions under public health surveillance. MMWR Morb Mortal Wkly Rep. 1997;46:1–55. - PubMed
-
- Glassroth J, Robins AG, Snider DE. Tuberculosis in the1980s. N Engl J Med. 1980;302:1441–50. - PubMed
-
- Woods AC. Modern concepts of the etiology of uveitis. Am J Ophthalmol. 1960;50:1170–87. - PubMed
-
- Kazokoglu H, Onal S, Tugal-Tutkun I, Mirza E, Akova Y, Ozyazgan Y, et al. Demographic and clinical features of uveitis in tertiary centers in Turkey. Ophthalmic Epidemiol. 2008;15:285–93. - PubMed
LinkOut - more resources
Full Text Sources
