

Emergent infectious uveitis
- PMID: 20404989
- PMCID: PMC2855663
- DOI: 10.4103/0974-9233.58426
Emergent infectious uveitis
Abstract
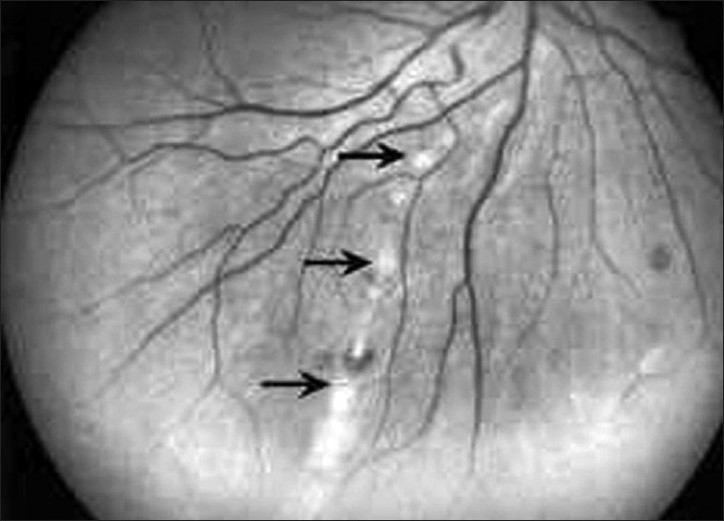
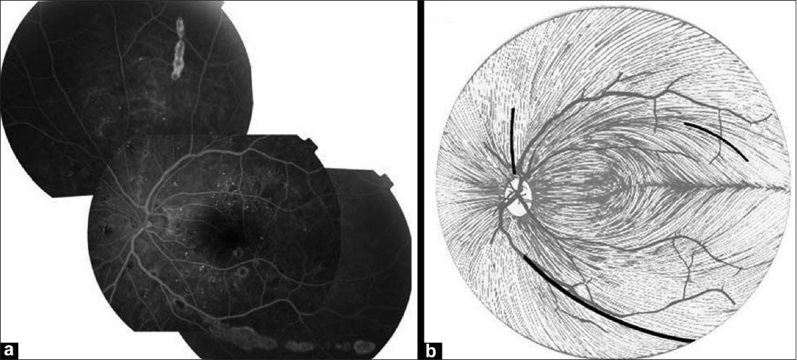
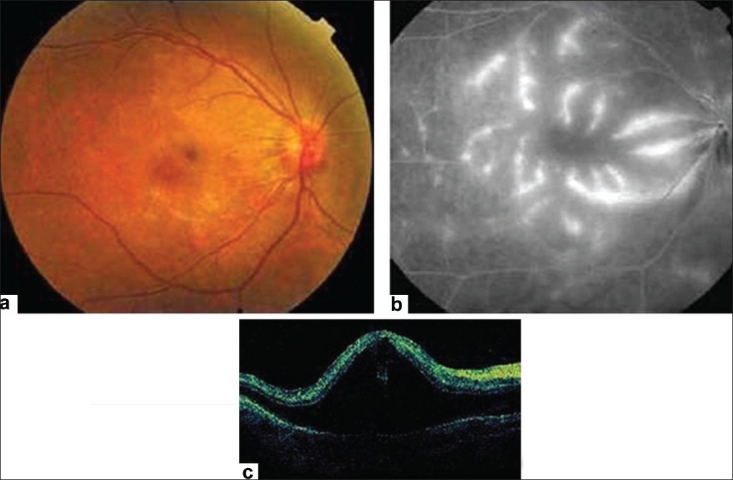
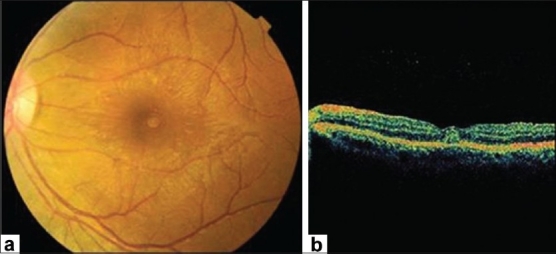
Infectious causes should always be considered in all patients with uveitis and it should be ruled out first. The differential diagnosis includes multiple well-known diseases including herpes, syphilis, toxoplasmosis, tuberculosis, bartonellosis, Lyme disease, and others. However, clinicians should be aware of emerging infectious agents as potential causes of systemic illness and also intraocular inflammation. Air travel, immigration, and globalization of business have overturned traditional pattern of geographic distribution of infectious diseases, and therefore one should work locally but think globally, though it is not possible always. This review recapitulates the systemic and ocular mainfestations of several emergent infectious diseases relevant to the ophthalmologist including Rickettsioses, West Nile virus infection, Rift valley fever, dengue fever, and chikungunya. Retinitis, chorioretinitis, retinal vasculitis, and optic nerve involvement have been associated with these emergent infectious diseases. The diagnosis of any of these infections is usually based on pattern of uveitis, systemic symptoms and signs, and specific epidemiological data and confirmed by detection of specific antibody in serum. A systematic ocular examination, showing fairly typical fundus findings, may help in establishing an early clinical diagnosis, which allows prompt, appropriate management.
Keywords: Infectious Disease; Systemic Illness; Uveitis.
Conflict of interest statement
Figures


Similar articles
-
Novel infectious agents causing uveitis.Int Ophthalmol. 2010 Oct;30(5):465-83. doi: 10.1007/s10792-009-9319-6. Epub 2009 Aug 27. Int Ophthalmol. 2010. PMID: 19711015 Review.
-
Ocular Manifestations of Emerging Arthropod-Borne Infectious Diseases.J Curr Ophthalmol. 2021 Oct 22;33(3):227-235. doi: 10.4103/joco.joco_134_21. eCollection 2021 Jul-Sep. J Curr Ophthalmol. 2021. PMID: 34765808 Free PMC article. Review.
-
New infectious etiologies for posterior uveitis.Ophthalmic Res. 2013;49(2):66-72. doi: 10.1159/000344009. Epub 2012 Dec 18. Ophthalmic Res. 2013. PMID: 23258387 Review.
-
Ocular manifestations of emerging infectious diseases.Curr Opin Ophthalmol. 2013 Nov;24(6):574-80. doi: 10.1097/ICU.0b013e3283654e09. Curr Opin Ophthalmol. 2013. PMID: 24030241 Review.
-
[Tropical ophthalmology : Intraocular inflammation caused by "new" infectious pathogens and travel-related infections].Ophthalmologe. 2016 Jan;113(1):35-46. doi: 10.1007/s00347-015-0176-6. Ophthalmologe. 2016. PMID: 26649438 Review. German.
Cited by
-
Rickettsial disease: An underestimated cause of posterior uveitis.Saudi J Ophthalmol. 2022 Dec 27;36(4):374-379. doi: 10.4103/sjopt.sjopt_86_22. eCollection 2022 Oct-Dec. Saudi J Ophthalmol. 2022. PMID: 36618574 Free PMC article.
-
14th EUNOS Congress: PORTO, PORTUGAL, 16-19 JUNE 2019.Neuroophthalmology. 2019 Jun 7;43(Suppl 1):1-221. doi: 10.1080/01658107.2019.1608780. eCollection 2019 Jun. Neuroophthalmology. 2019. PMID: 31528195 Free PMC article. No abstract available.
-
Current concepts and future directions in the pathogenesis and management of non infectious uveitis.Eye (Lond). 2012 Jun;26(6):890; author reply 890-1. doi: 10.1038/eye.2012.44. Epub 2012 Mar 9. Eye (Lond). 2012. PMID: 22402702 Free PMC article. No abstract available.
-
Potential for autoimmune pathogenesis of Rift Valley Fever virus retinitis.Am J Trop Med Hyg. 2013 Sep;89(3):495-7. doi: 10.4269/ajtmh.12-0562. Epub 2013 Aug 5. Am J Trop Med Hyg. 2013. PMID: 23918215 Free PMC article.
-
Management of presumed trematode induced granulomatous uveitis in pediatric patients.Jpn J Ophthalmol. 2019 Jan;63(1):119-125. doi: 10.1007/s10384-018-0632-3. Epub 2018 Nov 2. Jpn J Ophthalmol. 2019. PMID: 30386949
References
-
- Parola P, Raoult D. Rickettsioses eruptives. EMC (Elsevier Paris) Maladies infectieuses. 1998;8-037-I-20:24.
-
- McDade JE. Rickettsial diseases. In: Hausler WJ, Sussman M, editors. Topley and Wilson's Microbiology and Microbial Infections. 9 th ed. London: London; 1998. pp. 995–1011.
-
- Alio J, Ruiz-Beltran R, Herrero-Herrero JI, Hernandez E. Retinal manifestations of Mediterranean spotted fever. Ophthalmologica. 1987;195:31–7. - PubMed
-
- Khairallah M, Ladjimi A, Chakroun M, Messaoud R, Ben Yahia S, Zaouali S, et al. Posterior segment manifestations of Rickettsia conorii infection. Ophthalmology. 2004;111:529–34. - PubMed
-
- Raab EL, Leopold IH, Hodes HL. Retinopathy in Rocky Mountain spotted fever. Am J Ophthalmol. 1969;68:42–6. - PubMed
LinkOut - more resources
Full Text Sources
