

Inflammatory choroidal neovascularization
- PMID: 20404991
- PMCID: PMC2855665
- DOI: 10.4103/0974-9233.58422
Inflammatory choroidal neovascularization
Abstract
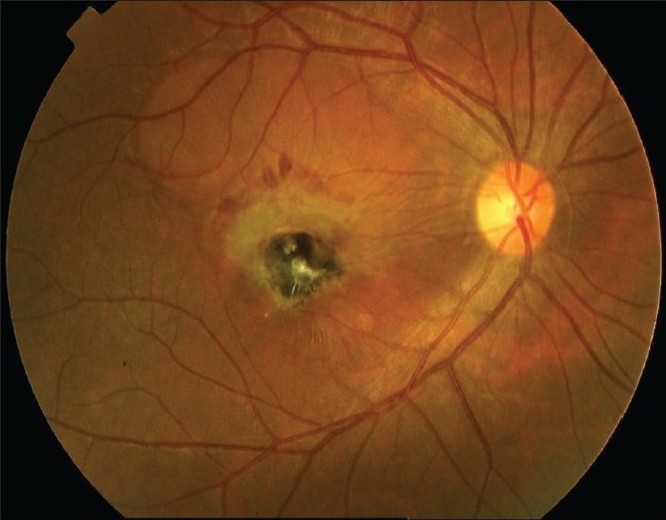
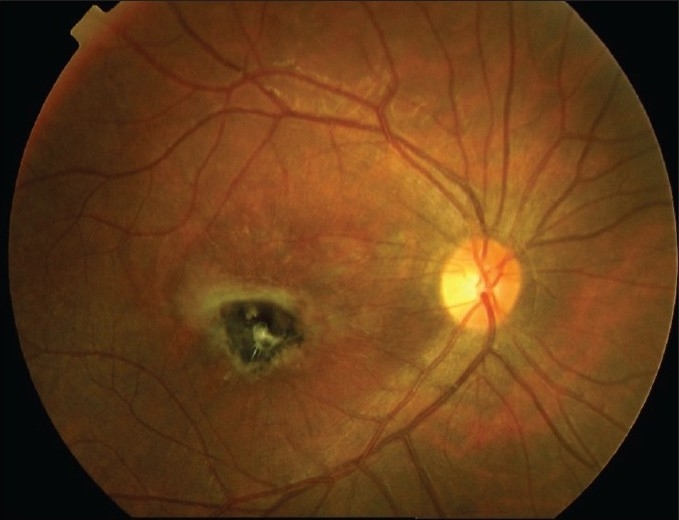
Purpose and methods: Choroidal neovascularization (CNV) can be a severe sight-threatening sequela, which can be secondary to both infectious and noninfectious uveitis. This review summarizes the different diseases associated with CNV, highlighting new treatment modalities and the possible strategies, which could be applied for the therapy of this occurrence.
Results: Since CNV can often originate from posterior pole lesions and can be hard to identify, an accurate examination is mandatory in order to identify the correct diagnosis. In the majority of cases, fluorescein angiography (FA), indocyanine green angiography (ICGA) and optical coherence tomography (OCT) enable the determination of the clinical characteristics of the CNV. An infectious disease should be looked for to include a suitable therapy when available. The treatment strategy for CNV secondary to noninfectious uveal inflammations should be directed at controlling the inflammatory process. Systemic corticosteroids with or without immunosuppressive agents are indicated even when the CNV occurs with apparently inactive uveitis: Chronic subclinical inflammation can be the basis for the pathogenesis of CNV. Additional therapies aimed directly at the neovascular process, such as the intravitreal anti-Vascular Endothelial Growth Factor (VEGF) agents, are recommended particularly when the therapy shows an insufficient response.
Conclusion: CNV secondary to uveitis is a severe sequela leading to significant visual impairment. ICGA is mandatory in order to obtain relevant information about the choroidal status. Several therapeutic options have been considered, but no guidelines are provided at the moment. Moreover, the current data are still only based on case reports or small series. For such reasons, further trials are mandatory to validate the preliminary available results.
Keywords: Choroidal Neovascularization; Choroiditis; Immunosuppression; Steroids; Uveitis; Vascular Endothelial Growth Factor.
Conflict of interest statement
Figures

References
-
- Glaser BM, Campochiaro PA, Davis JL JL, Jr, Jerdan JA. Retinal pigment epithelial cells release inhibitors of neovascularization. Ophthalmology. 1987;94:780–4. - PubMed
-
- Wong HC, Boulton M, McLeod D, Bayly M, Clark P, Marshall J. Retinal pigment epithelium in culture produce retinal vascular mitogens. Arch Ophthalmol. 1988;106:1439–43. - PubMed
-
- Ambati J, Ambati BK, Yoo SH, Ianchulev S, Adamis AP. Age-related macular degeneration Etiology, pathogenesis, and therapeutic strategies. Surv Ophthalmol. 2003;48:257–93. - PubMed
-
- Forrester JV, Liversidge J, Dua HS, Towler H, McMenamin PG. Comparison of clinical experimental uveitis. Curr Eye Res. 1990;9:75–84. - PubMed
-
- Grossniklaus HE, Gass JD. Clinicopathologic correlations of surgically excised type 1 and type 2 submacular choroidal neovascular membranes. Am J Ophthalmol. 1998;126:59–69. - PubMed
LinkOut - more resources
Full Text Sources
