

Measuring under-five mortality: validation of new low-cost methods
- PMID: 20405055
- PMCID: PMC2854123
- DOI: 10.1371/journal.pmed.1000253
Measuring under-five mortality: validation of new low-cost methods
Abstract
Background: There has been increasing interest in measuring under-five mortality as a health indicator and as a critical measure of human development. In countries with complete vital registration systems that capture all births and deaths, under-five mortality can be directly calculated. In the absence of a complete vital registration system, however, child mortality must be estimated using surveys that ask women to report the births and deaths of their children. Two survey methods exist for capturing this information: summary birth histories and complete birth histories. A summary birth history requires a minimum of only two questions: how many live births has each mother had and how many of them have survived. Indirect methods are then applied using the information from these two questions and the age of the mother to estimate under-five mortality going back in time prior to the survey. Estimates generated from complete birth histories are viewed as the most accurate when surveys are required to estimate under-five mortality, especially for the most recent time periods. However, it is much more costly and labor intensive to collect these detailed data, especially for the purpose of generating small area estimates. As a result, there is a demand for improvement of the methods employing summary birth history data to produce more accurate as well as subnational estimates of child mortality.
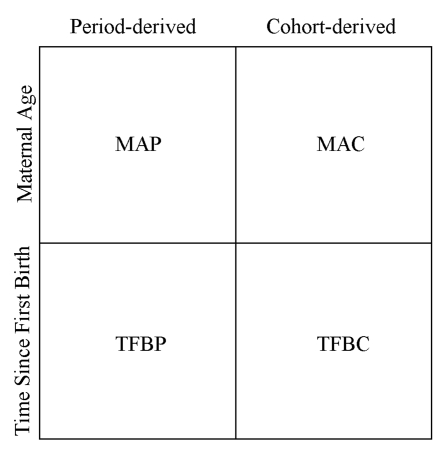
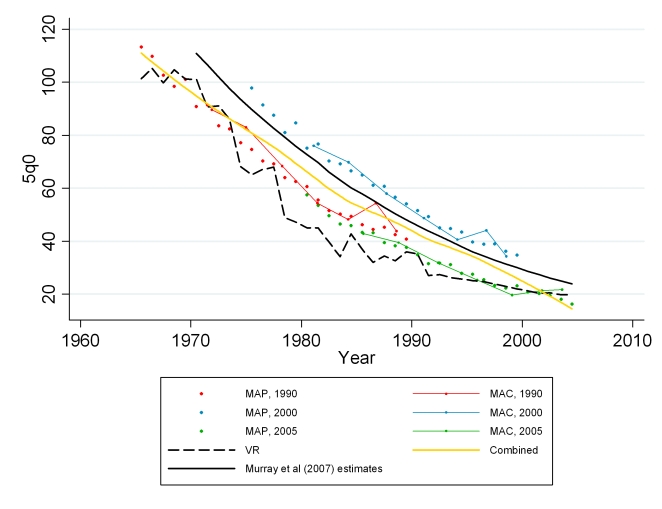
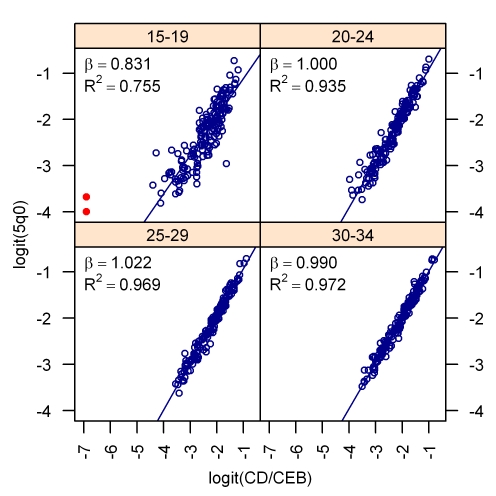
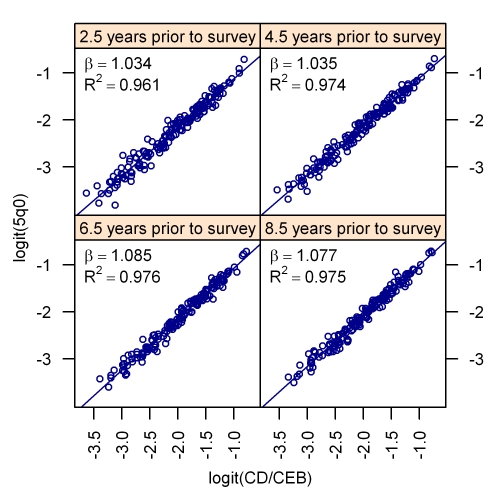
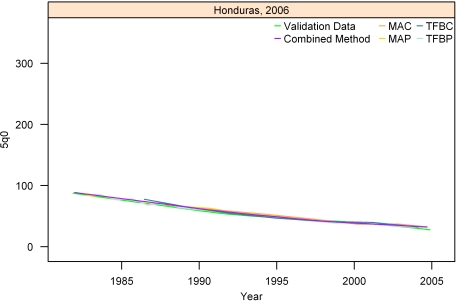
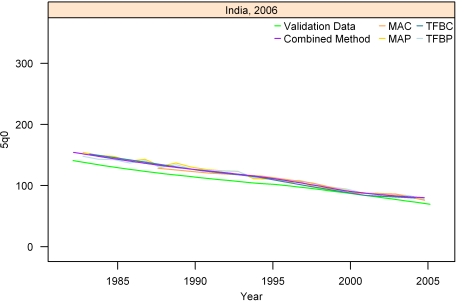
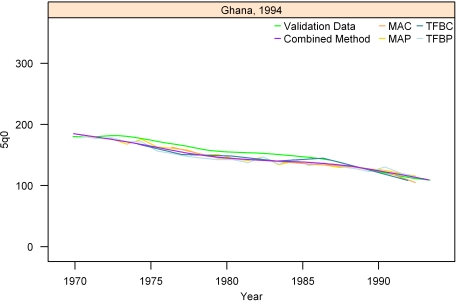
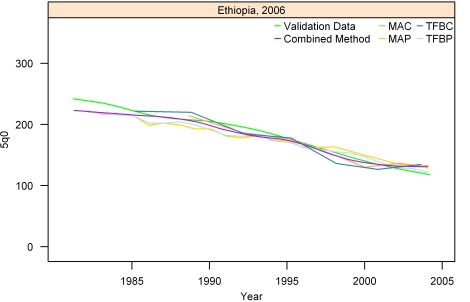
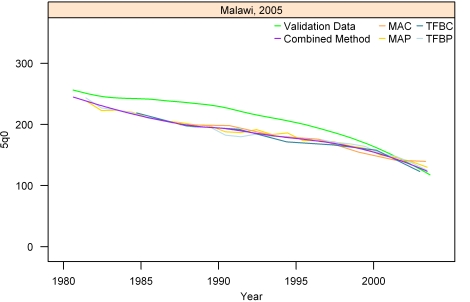
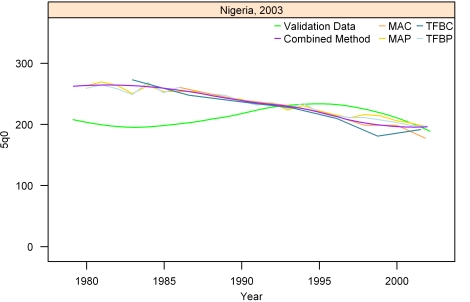
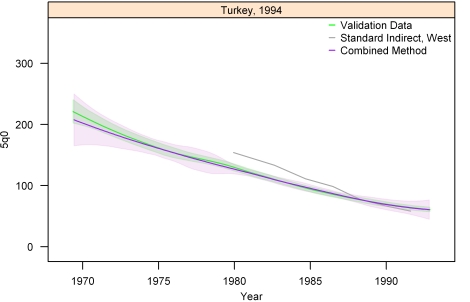
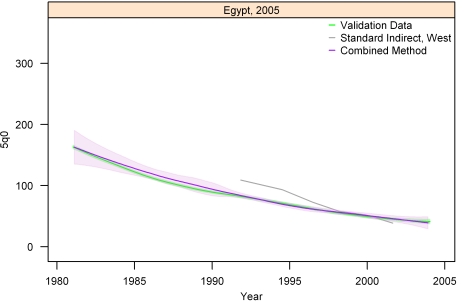
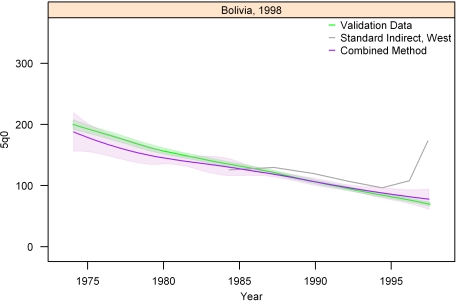
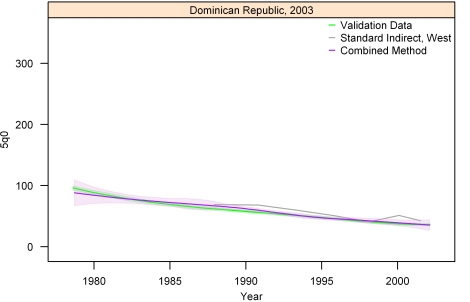
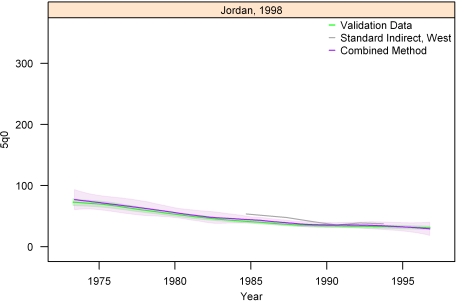
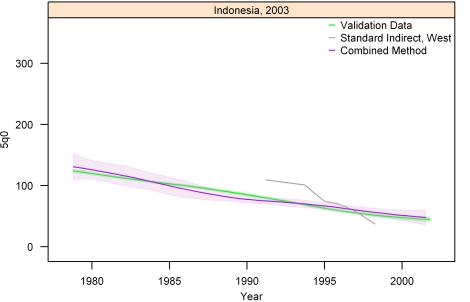
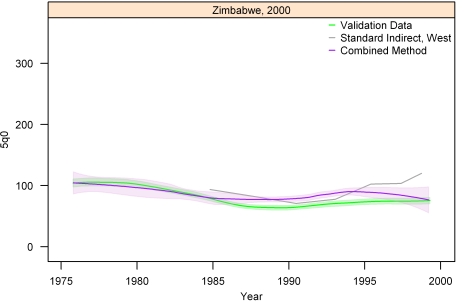
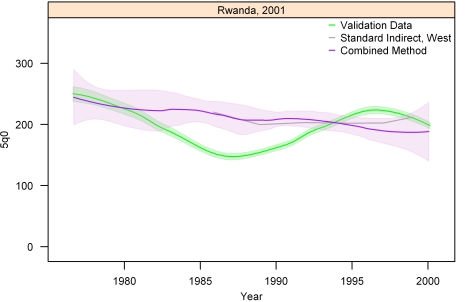
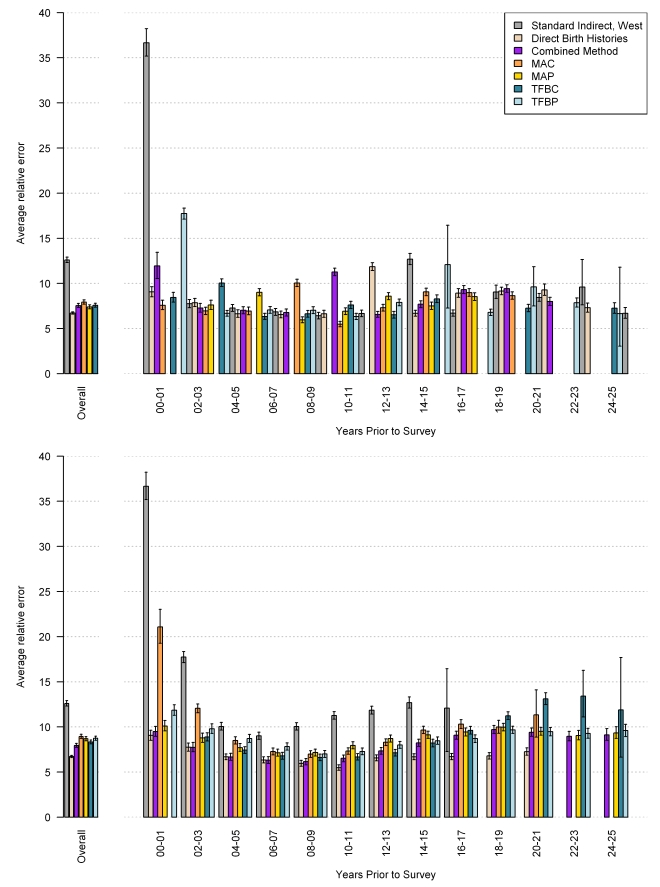
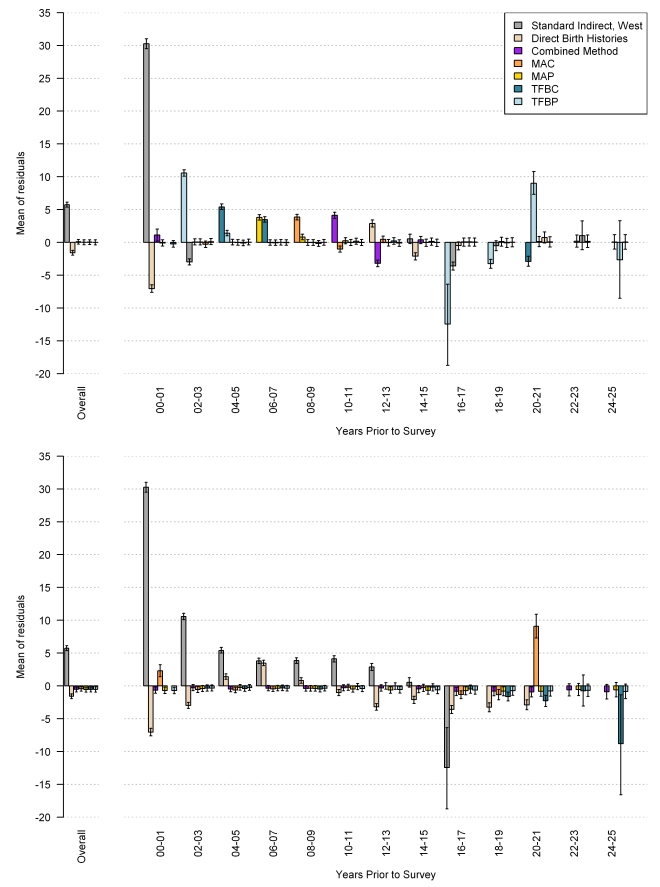
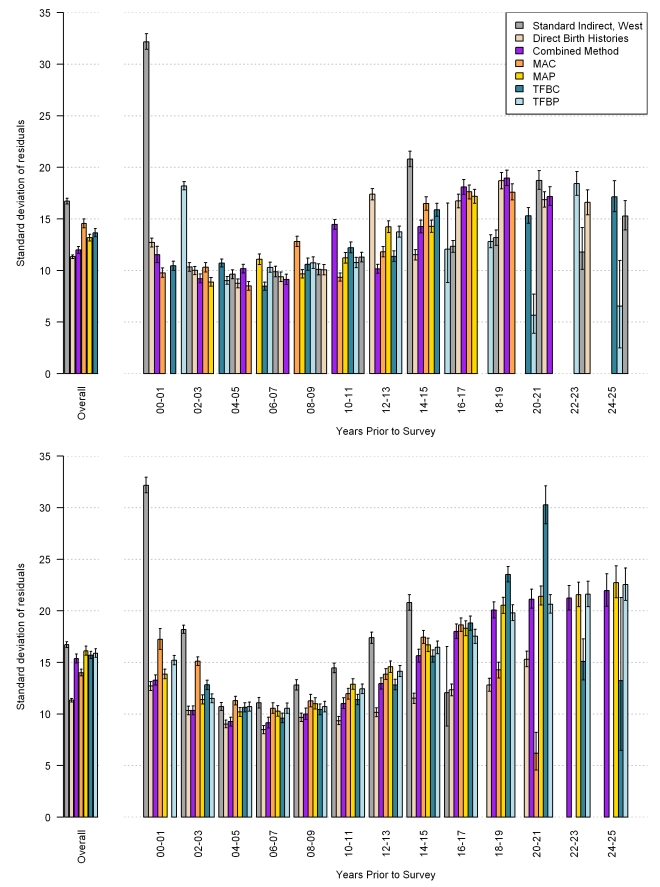
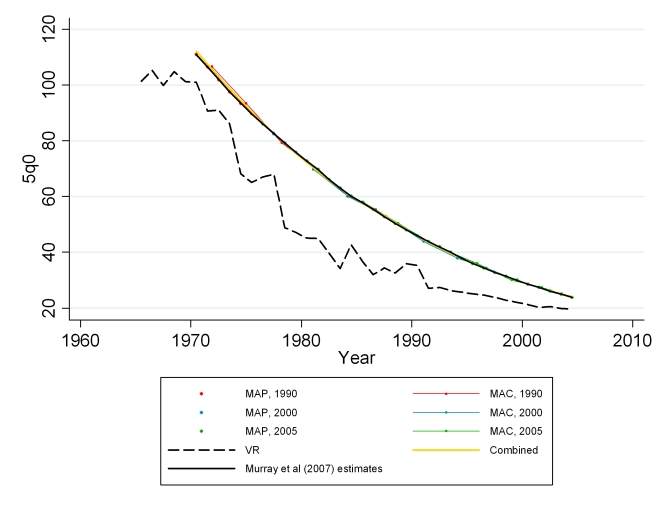
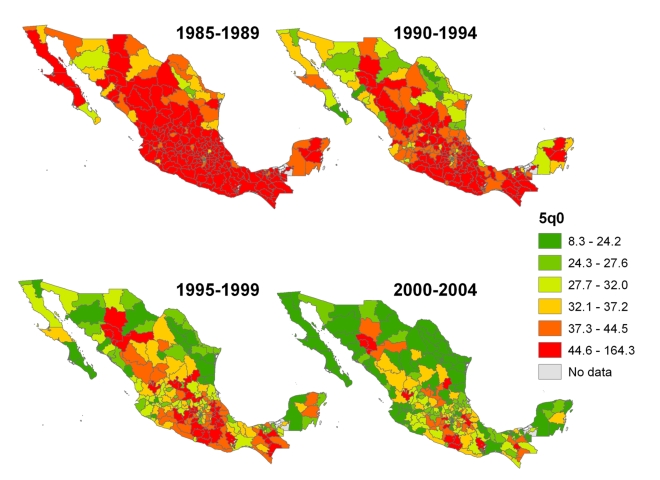
Methods and findings: We used data from 166 Demographic and Health Surveys (DHS) to develop new empirically based methods of estimating under-five mortality using children ever born and children dead data. We then validated them using both in- and out-of-sample analyses. We developed a range of methods on the basis of three dimensions of the problem: (1) approximating the average length of exposure to mortality from a mother's set of children using either maternal age or time since first birth; (2) using cohort and period measures of the fraction of children ever born that are dead; and (3) capturing country and regional variation in the age pattern of fertility and mortality. We focused on improving estimates in the most recent time periods prior to a survey where the traditional indirect methods fail. In addition, all of our methods incorporated uncertainty. Validated against under-five estimates generated from complete birth histories, our methods outperformed the standard indirect method by an average of 43.7% (95% confidence interval [CI] 41.2-45.2). In the 5 y prior to the survey, the new methods resulted in a 53.3% (95% CI 51.3-55.2) improvement. To illustrate the value of this method for local area estimation, we applied our new methods to an analysis of summary birth histories in the 1990, 2000, and 2005 Mexican censuses, generating subnational estimates of under-five mortality for each of 233 jurisdictions.
Conclusions: The new methods significantly improve the estimation of under-five mortality using summary birth history data. In areas without vital registration data, summary birth histories can provide accurate estimates of child mortality. Because only two questions are required of a female respondent to generate these data, they can easily be included in existing survey programs as well as routine censuses of the population. With the wider application of these methods to census data, countries now have the means to generate estimates for subnational areas and population subgroups, important for measuring and addressing health inequalities and developing local policy to improve child survival. Please see later in the article for the Editors' Summary.
Conflict of interest statement
Alan Lopez is on the Editorial Board of
Figures
References
-
- United Nations. World declaration on the survival, protection and development of children and plan of action for implementing the world declaration on the survival, protection and development of children in the 1990s: World summit for children. 1990. New York: UN Publications. Available: http://www.unicef.org/wsc/plan.htm. Accessed 27 August 2009. - PubMed
-
- Murray CJ, Laakso T, Shibuya K, Hill K, Lopez AD. Can we achieve Millennium Development Goal 4? New analysis of country trends and forecasts of under-5 mortality to 2015. Lancet. 2007;370:1040–1054. - PubMed
-
- Black RE, Morris SS, Bryce J. Where and why are 10 million children dying every year? Lancet. 2003;361:2226–2234. - PubMed
-
- Bryce J, el AS, Pariyo G, Lanata C, Gwatkin D, et al. Reducing child mortality: can public health deliver? Lancet. 2003;362:159–164. - PubMed
-
- Claeson M, Gillespie D, Mshinda H, Troedsson H, Victora CG. Knowledge into action for child survival. Lancet. 2003;362:323–327. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
