

Prophylactic anticoagulation to prevent venous thromboembolism in traumatic intracranial hemorrhage: a decision analysis
- PMID: 20406444
- PMCID: PMC2887195
- DOI: 10.1186/cc8980
Prophylactic anticoagulation to prevent venous thromboembolism in traumatic intracranial hemorrhage: a decision analysis
Abstract
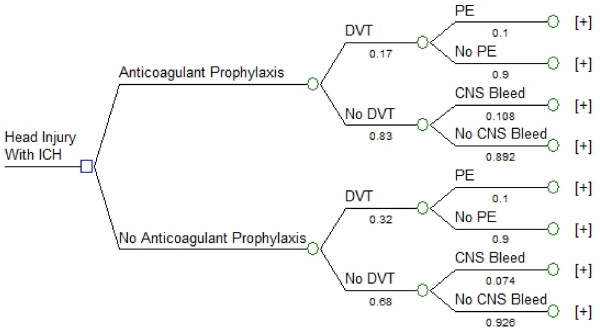
Introduction: Patients with intracranial hemorrhage due to traumatic brain injury are at high risk of developing venous thromboembolism including deep vein thrombosis (DVT) and pulmonary embolism (PE). Thus, there is a trade-off between the risks of progression of intracranial hemorrhage (ICH) versus reduction of DVT/PE with the use of prophylactic anticoagulation. Using decision analysis modeling techniques, we developed a model for examining this trade-off for trauma patients with documented ICH.
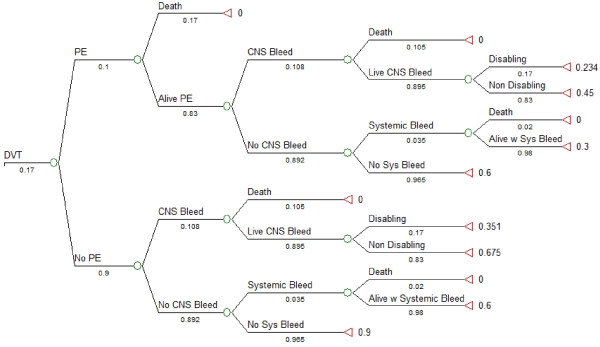
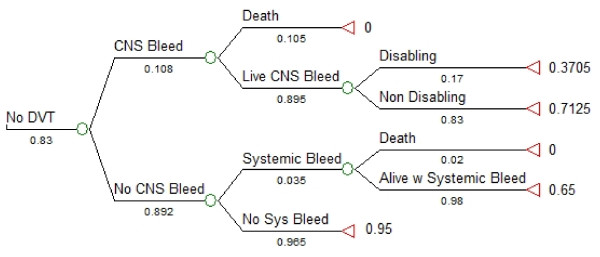
Methods: The decision node involved the choice to administer or to withhold low molecular weight heparin (LMWH) anticoagulation prophylaxis at 24 hours. Advantages of withholding therapy were decreased risk of ICH progression (death, disabling neurologic deficit, non-disabling neurologic deficit), and decreased risk of systemic bleeding complications (death, massive bleed). The associated disadvantage was greater risk of developing DVT/PE or death. Probabilities for each outcome were derived from natural history studies and randomized controlled trials when available. Utilities were obtained from accepted databases and previous studies.
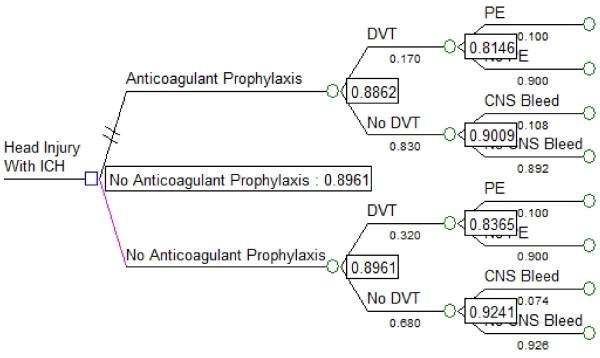
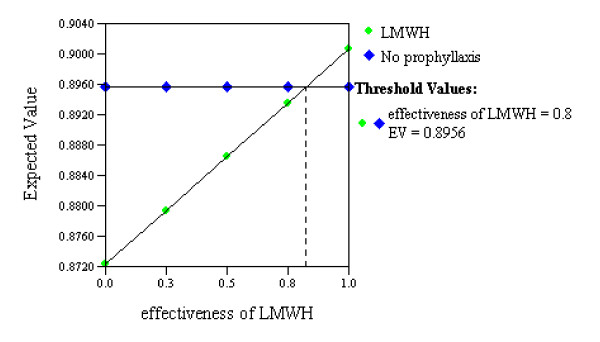
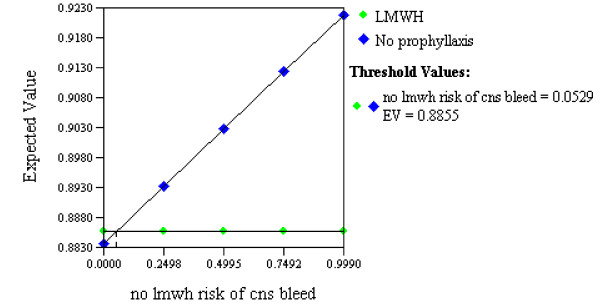
Results: The expected value associated with withholding anticoagulation prophylaxis was similar (0.90) to that associated with the LMWH strategy (0.89). Only two threshold values were encountered in one-way sensitivity analyses. If the effectiveness of LMWH at preventing DVT exceeded 80% (range from literature 33% to 82%) our model favoured this therapy. Similarly, our model favoured use of LMWH if this therapy increased the risk of ICH progression by no more than 5% above the baseline risk.
Conclusions: Our model showed no clear advantage to providing or withholding anticoagulant prophylaxis for DVT/PE prevention at 24 hours after traumatic brain injury associated with ICH. Therefore randomized controlled trials are justifiable and needed to guide clinicians.
Figures
Comment in
-
Preferences in traumatic intracranial hemorrhage: bleeding vs. clotting.Crit Care. 2010;14(3):153. doi: 10.1186/cc8996. Epub 2010 May 14. Crit Care. 2010. PMID: 20497598 Free PMC article.
References
-
- Servadei F, Murray GD, Teasdale GM, Dearden M, Iannotti F, Lapierre F, Maas AJ, Karimi A, Ohman J, Persson L, Stocchetti N, Trojanowski T, Unterberg A. Traumatic subarachnoid hemorrhage: demographic and clinical study of 750 patients from the European brain injury consortium survey of head injuries. Neurosurgery. 2002;50:261–267. doi: 10.1097/00006123-200202000-00006. - DOI - PubMed
-
- Gudeman SK, Kishore PR, Miller JD, Girevendulis AK, Lipper MH, Becker DP. The genesis and significance of delayed traumatic intracerebral hematoma. Neurosurgery. 1979;5:309–313. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
