

Differences in trauma team activation criteria among Norwegian hospitals
- PMID: 20406456
- PMCID: PMC2874509
- DOI: 10.1186/1757-7241-18-21
Differences in trauma team activation criteria among Norwegian hospitals
Abstract
Background: To ensure the rapid and correct triage of patients in potential need of specialized treatment, Norwegian hospitals are expected to establish trauma teams with predefined criteria for their activation. The objective of this study was to map and describe the criteria currently in use.
Methods: We undertook a cross-sectional survey in the summer of 2008, using structured telephone interviews to all Norwegian hospitals that might admit severely injured patients.
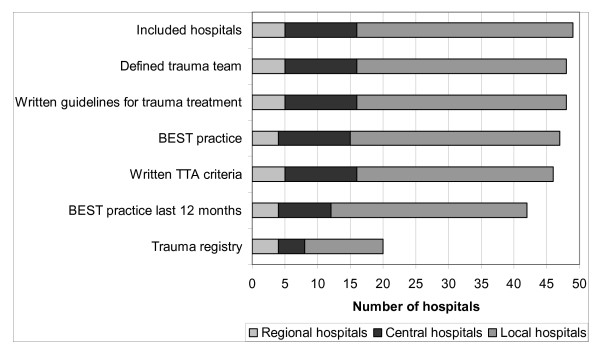
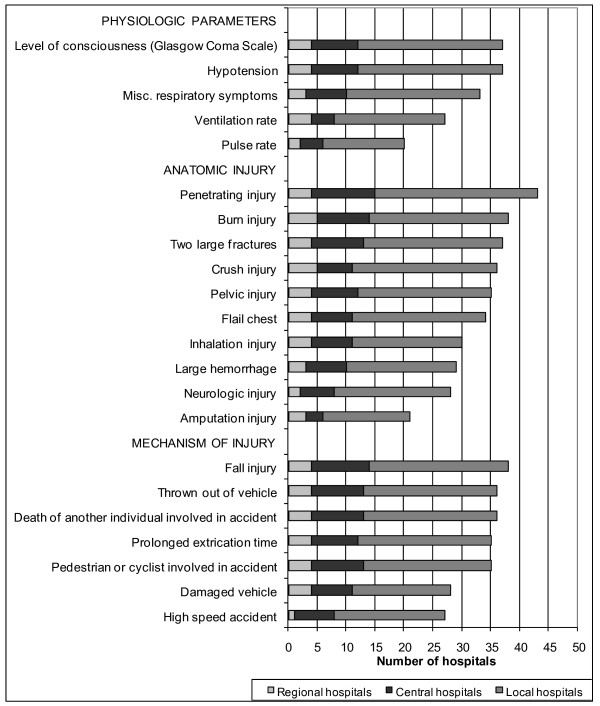
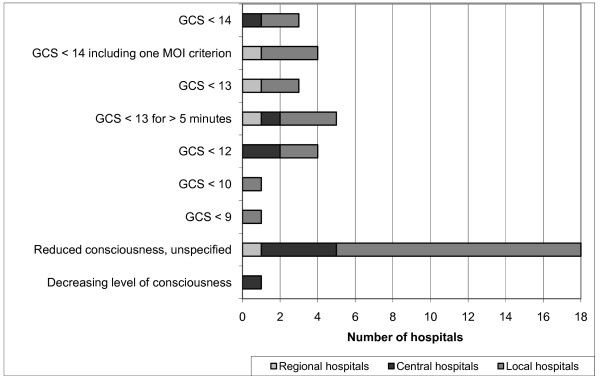
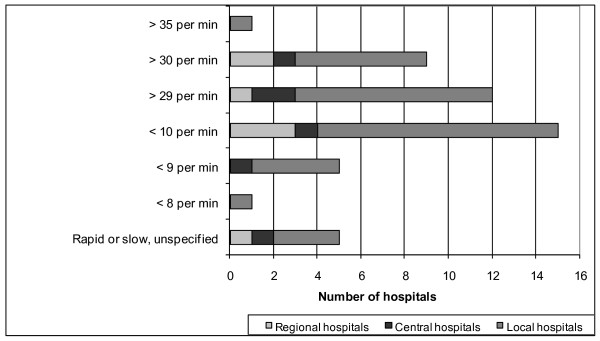
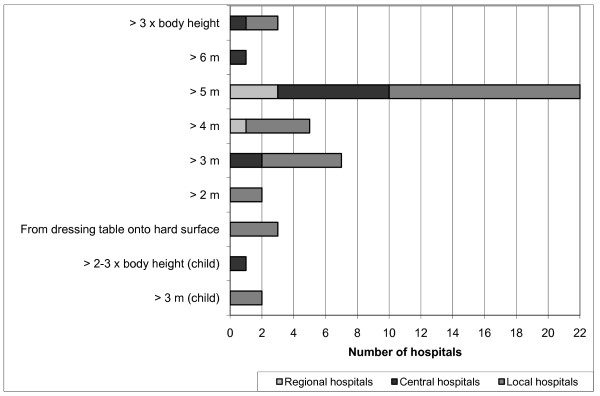
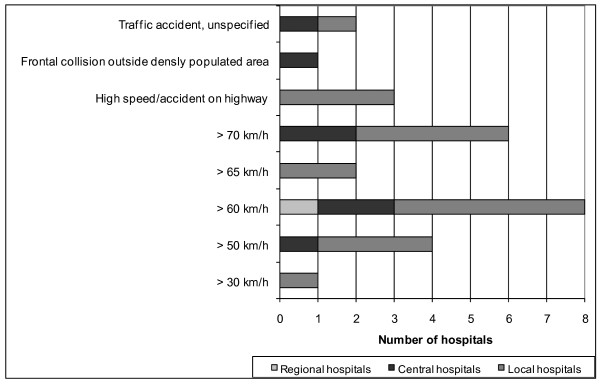
Results: Forty-nine hospitals were included, of which 48 (98%) had a trauma team and 20 had a hospital-based trauma registry. Criteria for trauma team activation were found at 46 (94%) hospitals. No single criterion was common to all hospitals. The median number of criteria per hospital was 23 (range 8-40), with a total number of 156 and wide variation with respect to physiological "cut-off" values. The mechanism of injury was commonly in use despite a well-known, large over-triage rate.
Conclusions: In recent years, Norwegian hospitals have gradually established trauma teams and criteria for their activation. These criteria show considerable variation, including physiological "cut-off" values.
Figures
References
-
- World Health Organization. The global burden of disease: 2004 update. . Geneva. 2004.
-
- American College of Surgeons. Optimal hospital resources for care of the seriously injured. Bull Am Coll Surg. 1976;61:15–22. - PubMed
-
- American College of Surgeons. Hospital and prehospital resources for the optimal care of the injured patient. Chicago, IL: American College of Surgeons; 1986.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
