

The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: prospective cohort study of 15 781 febrile illnesses
- PMID: 20406860
- PMCID: PMC2857748
- DOI: 10.1136/bmj.c1594
The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: prospective cohort study of 15 781 febrile illnesses
Abstract
Objectives: To evaluate current processes by which young children presenting with a febrile illness but suspected of having serious bacterial infection are diagnosed and treated, and to develop and test a multivariable model to distinguish serious bacterial infections from self limiting non-bacterial illnesses. Design Two year prospective cohort study. Setting The emergency department of The Children's Hospital at Westmead, Westmead, Australia.
Participants: Children aged less than 5 years presenting with a febrile illness between 1 July 2004 and 30 June 2006.
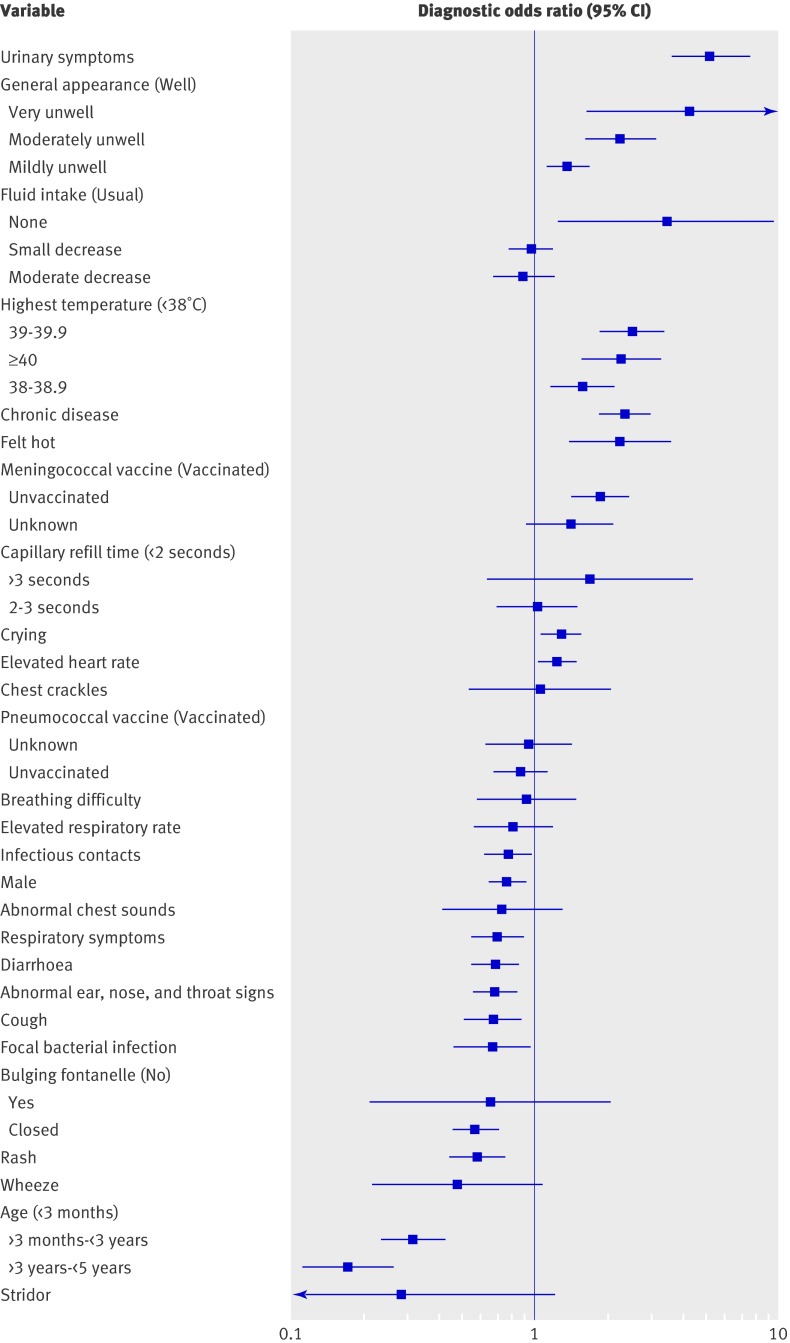
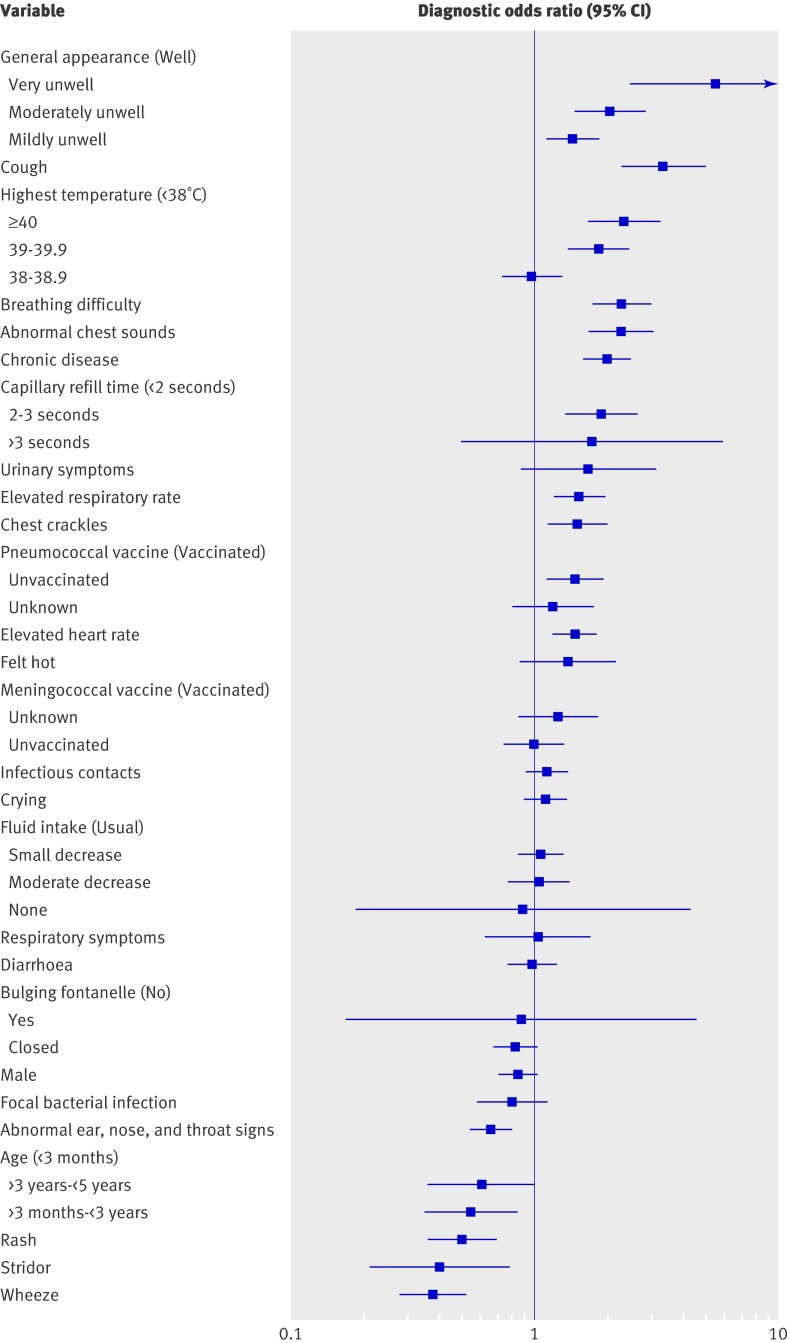
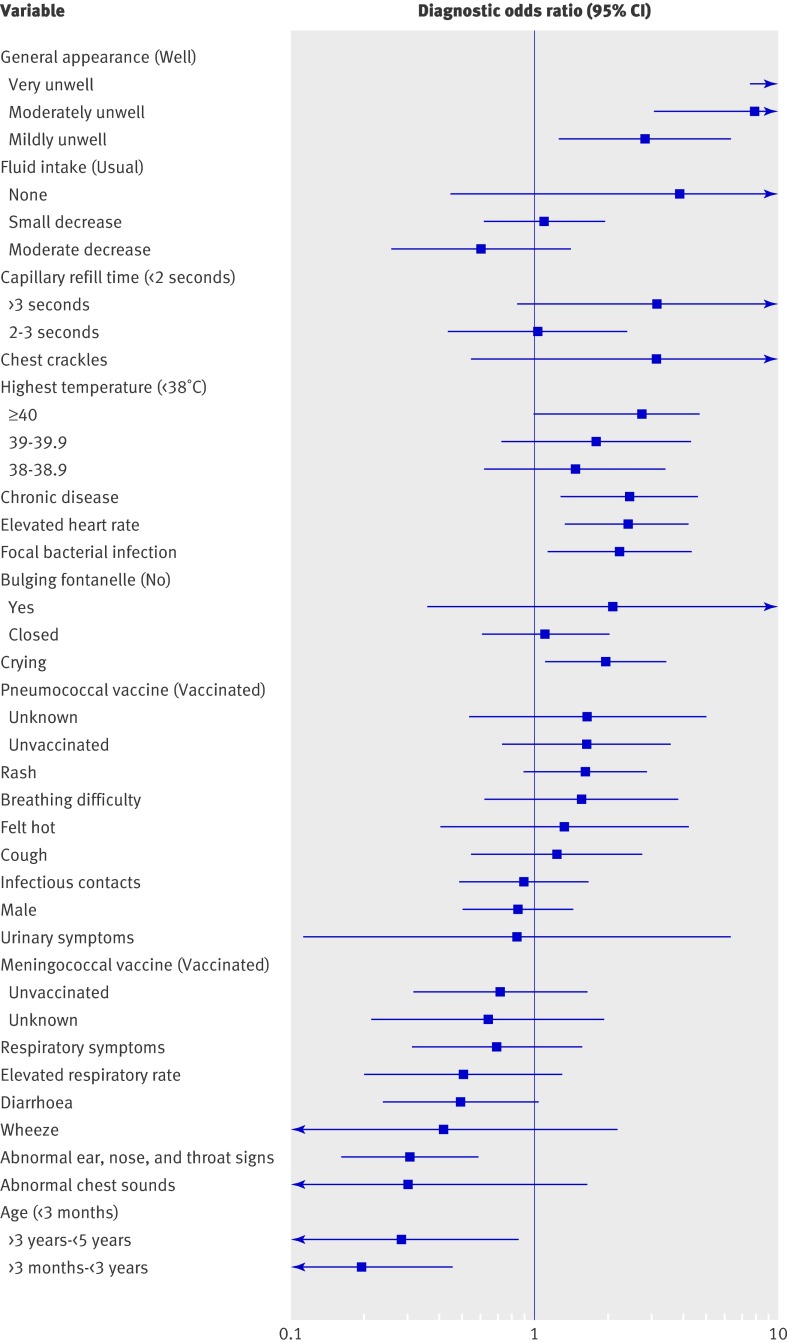
Intervention: A standardised clinical evaluation that included mandatory entry of 40 clinical features into the hospital's electronic record keeping system was performed by physicians. Serious bacterial infections were confirmed or excluded using standard radiological and microbiological tests and follow-up. Main outcome measures Diagnosis of one of three key types of serious bacterial infection (urinary tract infection, pneumonia, and bacteraemia), and the accuracy of both our clinical decision making model and clinician judgment in making these diagnoses.
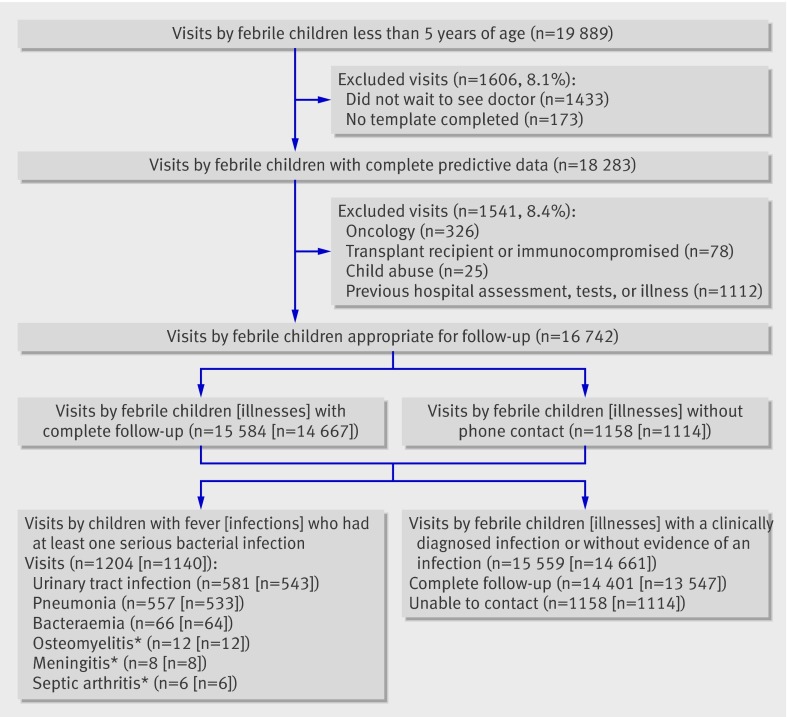
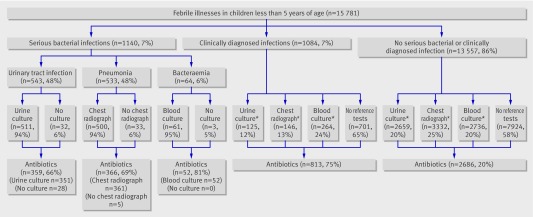
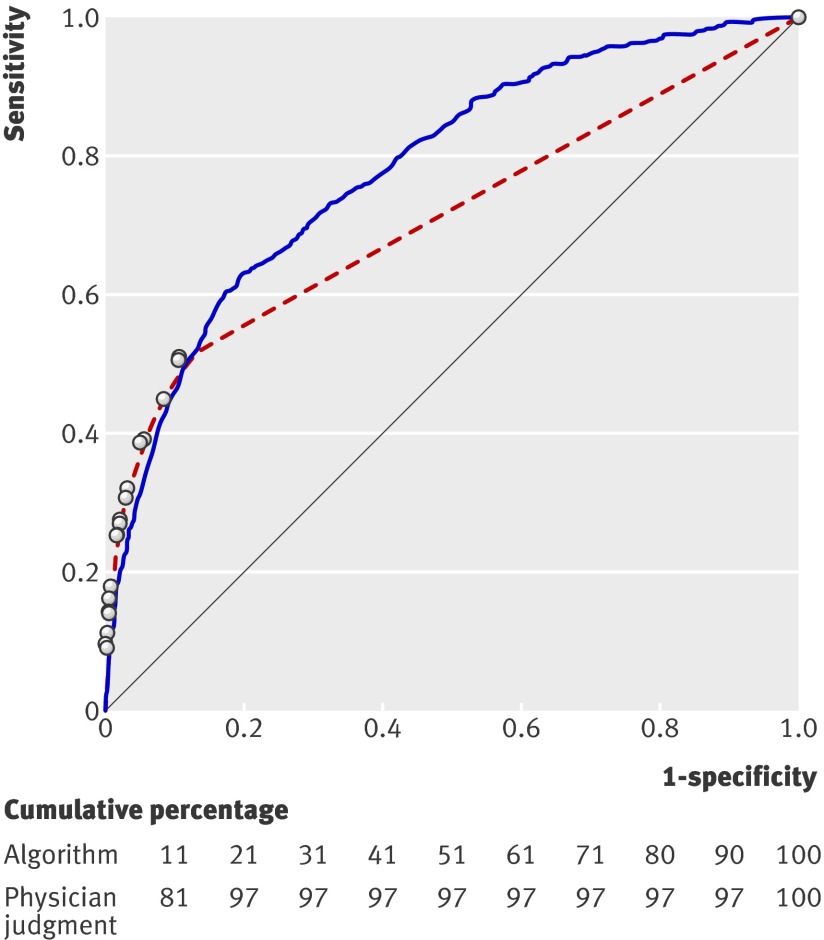
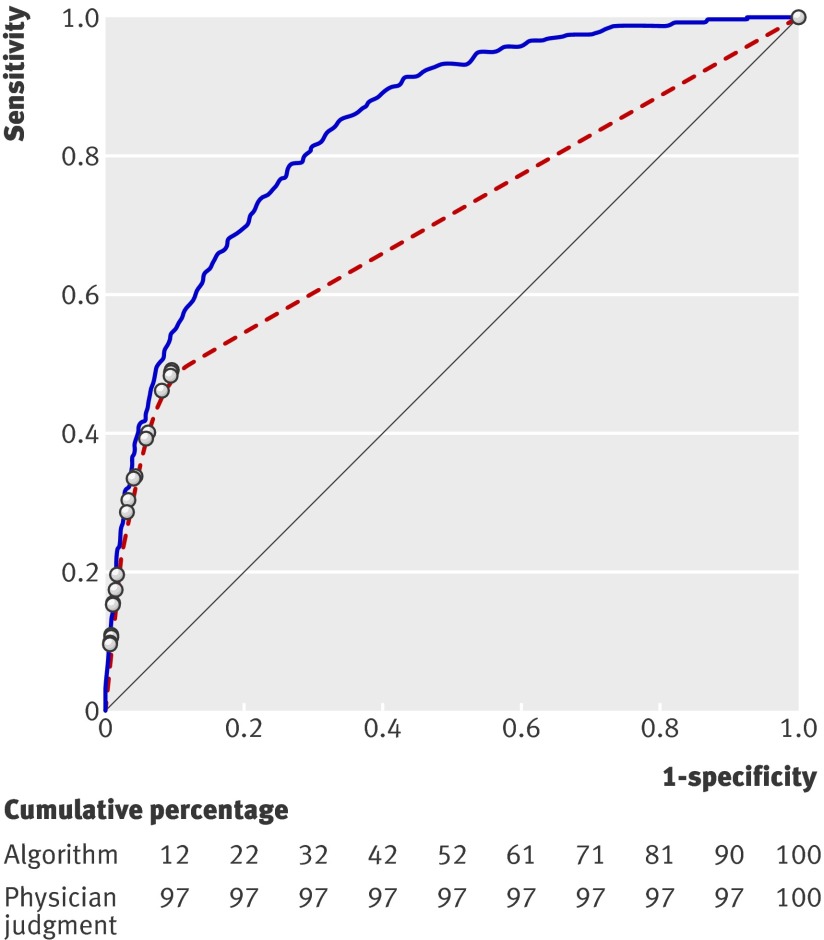
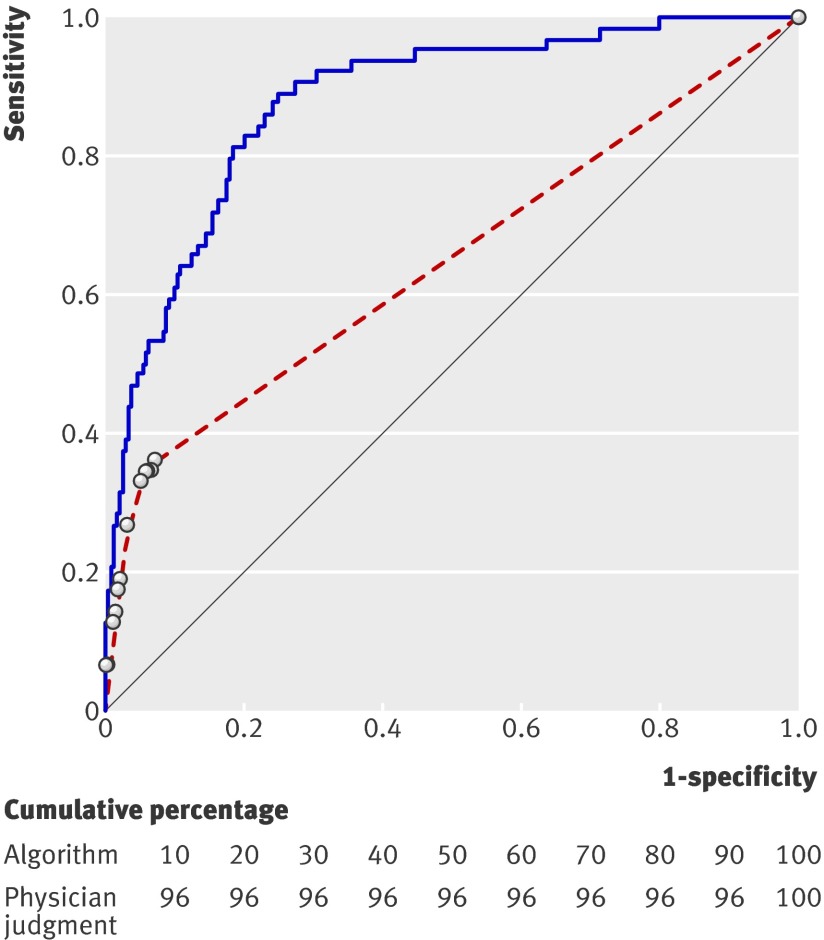
Results: We had follow-up data for 93% of the 15 781 instances of febrile illnesses recorded during the study period. The combined prevalence of any of the three infections of interest (urinary tract infection, pneumonia, or bacteraemia) was 7.2% (1120/15 781, 95% confidence interval (CI) 6.7% to 7.5%), with urinary tract infection the diagnosis in 543 (3.4%) cases of febrile illness (95% CI 3.2% to 3.7%), pneumonia in 533 (3.4%) cases (95% CI 3.1% to 3.7%), and bacteraemia in 64 (0.4%) cases (95% CI 0.3% to 0.5%). Almost all (>94%) of the children with serious bacterial infections had the appropriate test (urine culture, chest radiograph, or blood culture). Antibiotics were prescribed acutely in 66% (359/543) of children with urinary tract infection, 69% (366/533) with pneumonia, and 81% (52/64) with bacteraemia. However, 20% (2686/13 557) of children without bacterial infection were also prescribed antibiotics. On the basis of the data from the clinical evaluations and the confirmed diagnosis, a diagnostic model was developed using multinomial logistic regression methods. Physicians' diagnoses of bacterial infection had low sensitivity (10-50%) and high specificity (90-100%), whereas the clinical diagnostic model provided a broad range of values for sensitivity and specificity.
Conclusions: Emergency department physicians tend to underestimate the likelihood of serious bacterial infection in young children with fever, leading to undertreatment with antibiotics. A clinical diagnostic model could improve decision making by increasing sensitivity for detecting serious bacterial infection, thereby improving early treatment.
Conflict of interest statement
Conflicts of interest: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Diagnosing serious bacterial infection in young febrile children.BMJ. 2010 Apr 20;340:c2062. doi: 10.1136/bmj.c2062. BMJ. 2010. PMID: 20406862 No abstract available.
-
Diagnostic model appears to be more effective than clinical judgment in detecting serious bacterial infection in young febrile children.J Pediatr. 2010 Nov;157(5):862-3. doi: 10.1016/j.jpeds.2010.09.021. J Pediatr. 2010. PMID: 20955859 No abstract available.
References
-
- Hay AD. The prevalence of symptoms and consultations in pre-school children in the Avon Longitudinal Study of Parents and Children (ALSPAC): a prospective cohort study. Fam Pract 2005;22:367-74. - PubMed
-
- Schmitt BD. Fever phobia. Am J Dis Child 1980;134:176-81. - PubMed
-
- Heffernan R, Mostashari F, Das D, Karpati A, Kulldorf M, Weiss D. Syndromic surveillance in public health practice, New York City. Emerg Infect Dis 2004;10:858-64. - PubMed
-
- Alpern ER, Stanley RM, Gorelick MH, Donaldson A, Knight S, Teach SJ, et al. Epidemiology of pediatric emergency medicine research network. Pediatr Emerg Care 2006;22:689-99. - PubMed
-
- Massin MM, Montesanti J, Gerard P, Lepage P. Spectrum and frequency of illness presenting to a pediatric emergency department. Acta Clin Bel 2006;61;161-5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical