

Laparoscopic salvage total pelvic exenteration: Is it possible post-chemo-radiotherapy?
- PMID: 20407571
- PMCID: PMC2843126
- DOI: 10.4103/0972-9941.59310
Laparoscopic salvage total pelvic exenteration: Is it possible post-chemo-radiotherapy?
Abstract
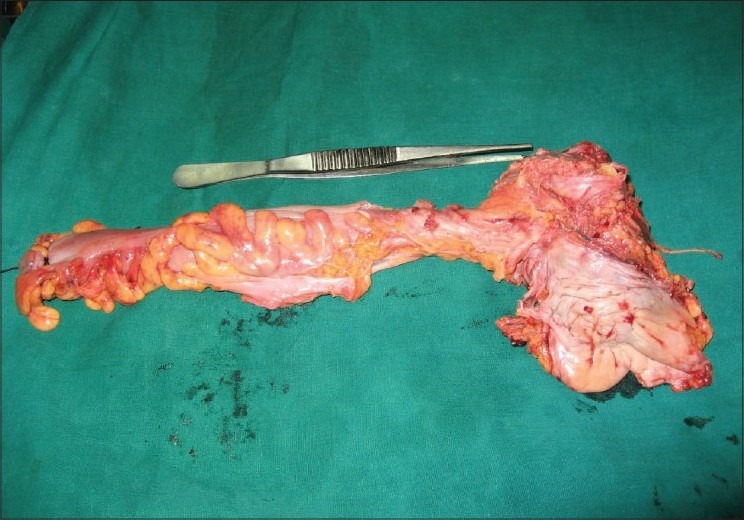
Indications for total pelvic exenteration in a male (removal of the bladder, prostate and rectum) and in a woman (removal bladder, uterus, vagina, ovaries and rectum) are rare. The advanced stage generally dictates that the patient has some form of chemotherapy or radiotherapy, or a combination of two to shrink/debulk the tumour. We report the first two cases of a salvage laparoscopic total pelvic exenteration in a male for rectal adenocarcinoma invading into the bladder and prostate, post-chemo-radiotherapy and in a woman for squamous cell carcinoma of cervix invading the bladder and rectum post-chemo-radiotherapy. Salvage surgery is often difficult and has been noted to have high morbidity. Applying a laparoscopic approach to this group may have advantages for the patient and the surgeon, i.e. less pain, early recovery and magnified views. As we have technically shown it to be possible, perhaps laparoscopic approaches should be discussed if the teams in these centres are of advanced laparoscopic surgeons working in multi-skilled groups.
Keywords: Laparoscopy; malignancy; pelvic exenteration.
Conflict of interest statement
Figures

References
-
- Brunschwig A. Complete excision of pelvic viscera for advanced carcinoma. Cancer. 1948;1:177–83. - PubMed
-
- Miller B, Morris M, Gershenson DM, Levenback CL, Burke TW. Intestinal fistulae formation following pelvic exenteration: A review of the University of Texas MD Anderson Cancer Center experience, 1957-1990. Gynecol Oncol. 1995;56:207–10. - PubMed
-
- Barber HR. Relative prognostic significance of preoperative and operative findings in pelvic exenteration. Surg Clin North Am. 1969;49:431–47. - PubMed
-
- Berek JS, Howe C, Lagasse LD, Hacker NF. Pelvic exenteration forrecurrent gynaecologic malignancy: Survival and morbidity analysis of the 45-year experience at UCLA. Gynecol Oncol. 2005;99:153–9. - PubMed
-
- Chi DS, Gemignani ML, Curtin JP, Hoskins WJ. Long-term experience in the surgical management of cancer of the uterine cervix. Semin Surg Oncol. 1999;17:161–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials