

Liver aminotransferases are elevated with rhabdomyolysis in the absence of significant liver injury
- PMID: 20407858
- PMCID: PMC3550495
- DOI: 10.1007/s13181-010-0075-9
Liver aminotransferases are elevated with rhabdomyolysis in the absence of significant liver injury
Abstract
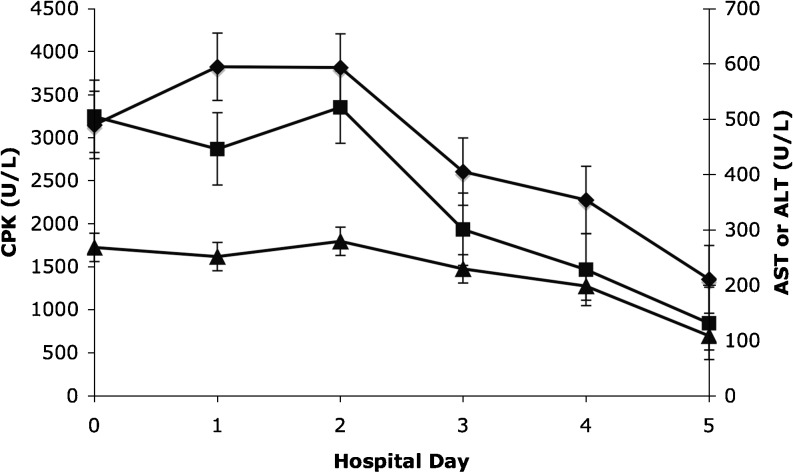
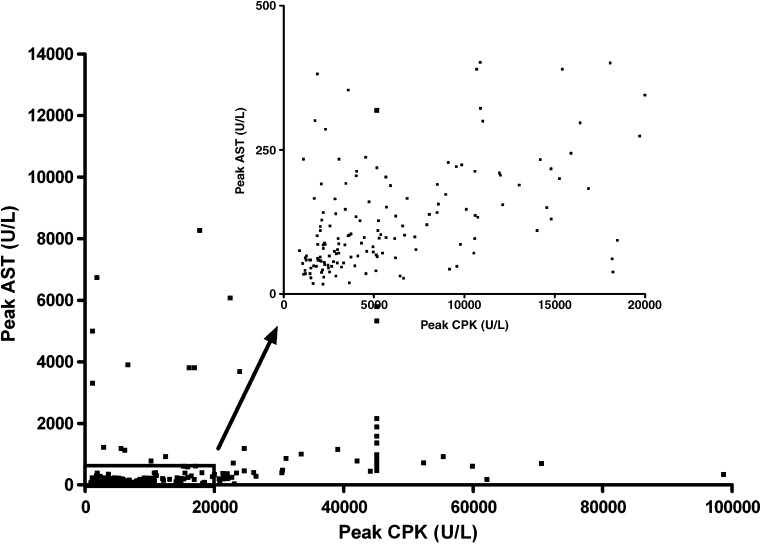
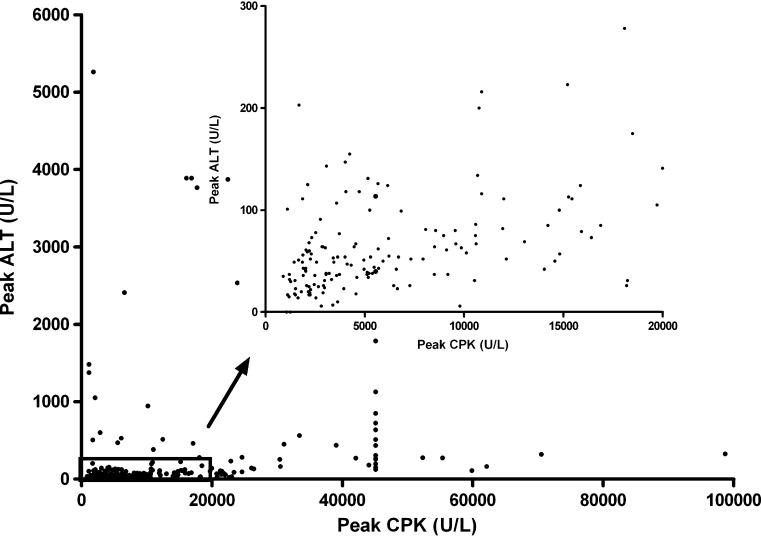
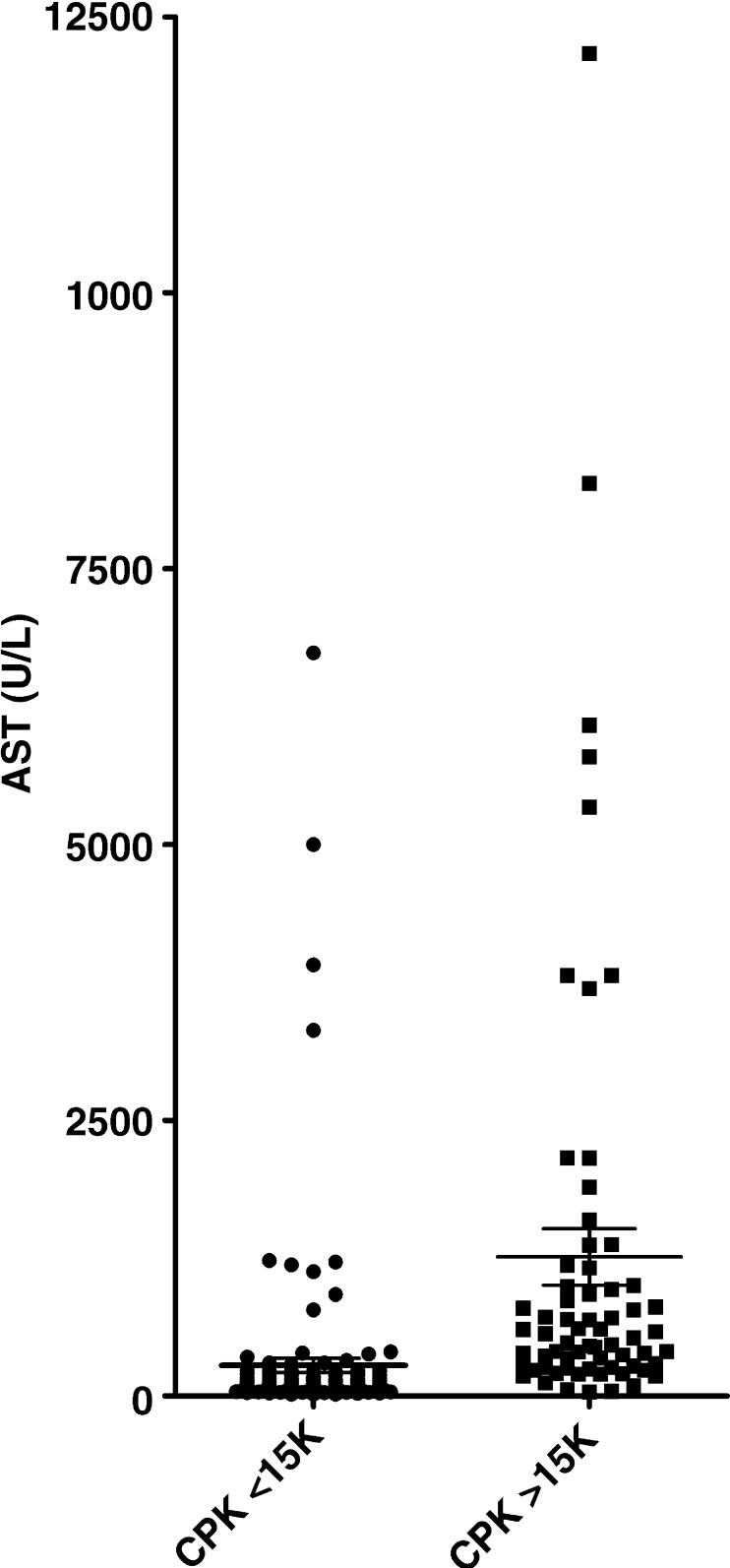
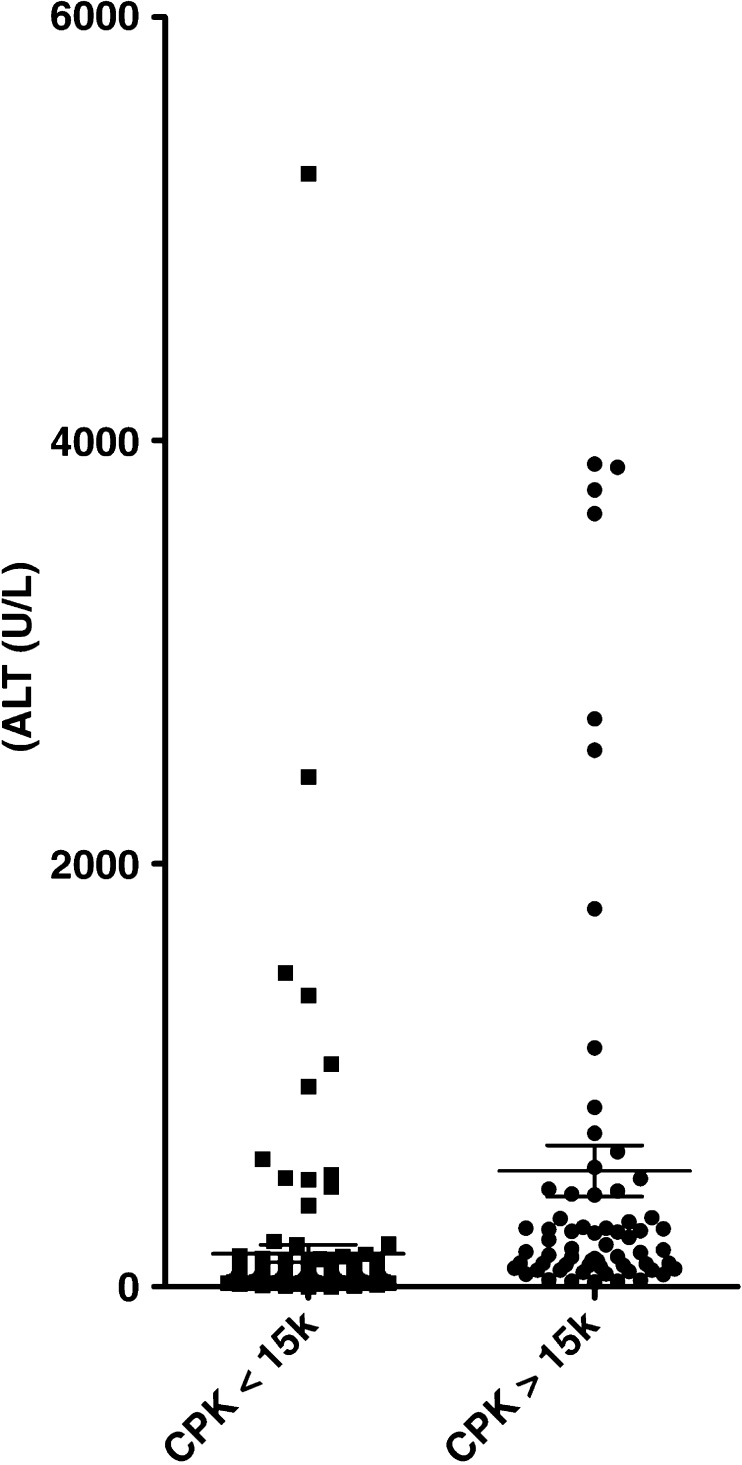
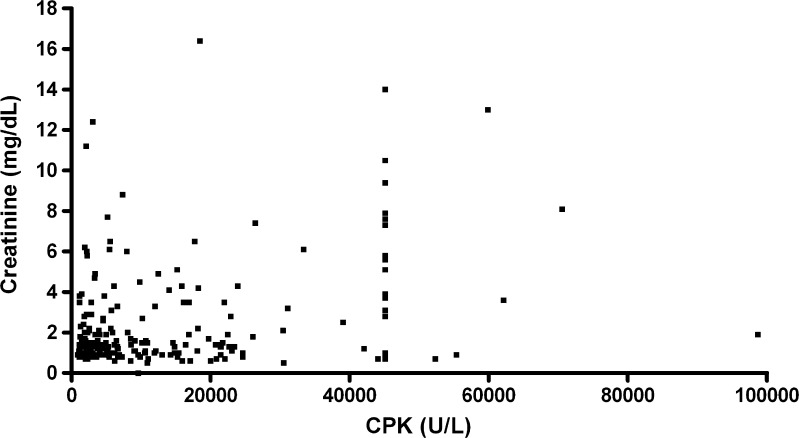
Rhabdomyolysis is an uncommon finding in the emergency department. However, the clinical implications of rhabdomyolysis are important, with a significant minority of patients developing acute renal failure and multiorgan failure. When present, the cause of elevated aminotransferases in the setting of rhabdomyolysis is often unclear. We sought to determine the incidence of abnormal aminotransferases (defined as aspartate aminotransferase (AST) or alanine aminotransferase (ALT)>40 U/L) in the setting of rhabdomyolysis and how the aminotransferases decrease relative to the creatine phosphokinase (CPK) concentration as rhabdomyolysis resolves. A retrospective chart review of 215 cases of rhabdomyolysis with CPK of >or=1,000 U/L was performed. The incidence of an abnormal AST in the setting of rhabdomyolysis was 93.1% (95% confidence interval, 88.7% to 95.8%). An abnormal ALT was much less common and found in 75.0% (95% confidence interval, 68.7% to 80.2%) of patients with a CPK of >or=1,000 U/L (p<0.0001). In only one instance was the ALT>40 U/L while the AST was <40 U/L. Furthermore, AST concentrations (and not ALT) fall in parallel with CPK during the first 6 days of hospitalization for patients with rhabdomyolysis. Aminotransferase abnormalities, particularly AST, are common in the setting of rhabdomyolysis. AST concentrations decrease in parallel to CPK, suggesting skeletal muscle may be a significant source of AST elevation in these patients.
Figures
Similar articles
-
Diagnosis and Management of Rhabdomyolysis in the Absence of Creatine Phosphokinase: A Medical Record Review.Mil Med. 2019 Dec 1;184(11-12):820-825. doi: 10.1093/milmed/usz101. Mil Med. 2019. PMID: 31090905 Review.
-
Role of Elevated Aminotransferases in ICU Patients with Rhabdomyolysis.Am Surg. 2015 Dec;81(12):1209-15. Am Surg. 2015. PMID: 26736155
-
Serum Aminotransferase Level in Rhabdomyolysis according to Concurrent Liver Disease.Korean J Gastroenterol. 2019 Oct 25;74(4):205-211. doi: 10.4166/kjg.2019.74.4.205. Korean J Gastroenterol. 2019. PMID: 31650796
-
Rhabdomyolysis among acute human poisoning cases.Hum Exp Toxicol. 2007 Jul;26(7):557-61. doi: 10.1177/0960327107078667. Hum Exp Toxicol. 2007. PMID: 17884958
-
Abnormal liver function tests associated with severe rhabdomyolysis.World J Gastroenterol. 2020 Mar 14;26(10):1020-1028. doi: 10.3748/wjg.v26.i10.1020. World J Gastroenterol. 2020. PMID: 32205993 Free PMC article. Review.
Cited by
-
Adverse effects of low-dose systemic cyclosporine therapy in high-risk penetrating keratoplasty.Graefes Arch Clin Exp Ophthalmol. 2015 Jul;253(7):1111-9. doi: 10.1007/s00417-015-3008-0. Epub 2015 Apr 21. Graefes Arch Clin Exp Ophthalmol. 2015. PMID: 25896110
-
Rhabdomyolysis Caused by Isotretinoin and Exercise in an Otherwise Healthy Female Patient.Cureus. 2022 Jun 15;14(6):e25981. doi: 10.7759/cureus.25981. eCollection 2022 Jun. Cureus. 2022. PMID: 35859962 Free PMC article.
-
Rhabdomyolysis in an unsuspecting patient.J Community Hosp Intern Med Perspect. 2018 Dec 28;8(6):386-388. doi: 10.1080/20009666.2018.1536243. eCollection 2018. J Community Hosp Intern Med Perspect. 2018. PMID: 31231482 Free PMC article.
-
Predicting and grading liver injury in the absence of computed tomographic imaging.J Family Med Prim Care. 2023 Feb;12(2):326-331. doi: 10.4103/jfmpc.jfmpc_1532_22. Epub 2023 Feb 28. J Family Med Prim Care. 2023. PMID: 37091021 Free PMC article.
-
A longitudinal rat forelimb model for assessing in vivo neuromuscular function following extremity reperfusion injury.Res Sq [Preprint]. 2025 Jan 29:rs.3.rs-5582098. doi: 10.21203/rs.3.rs-5582098/v1. Res Sq. 2025. PMID: 39975916 Free PMC article. Preprint.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
