

Survival in rectal cancer is predicted by T cell infiltration of tumour-associated lymphoid nodules
- PMID: 20408858
- PMCID: PMC2940152
- DOI: 10.1111/j.1365-2249.2010.04147.x
Survival in rectal cancer is predicted by T cell infiltration of tumour-associated lymphoid nodules
Abstract
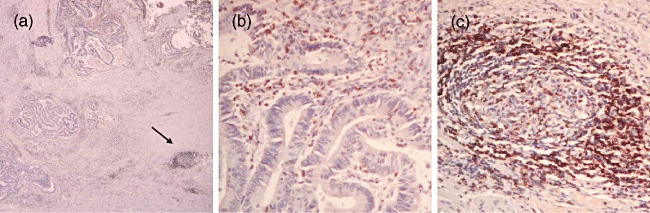
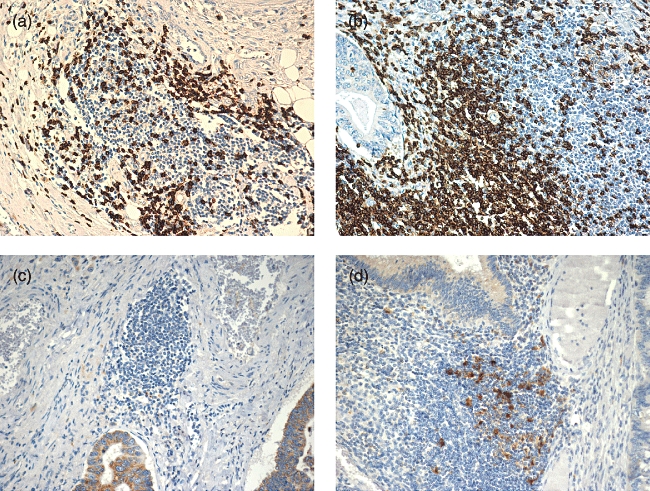
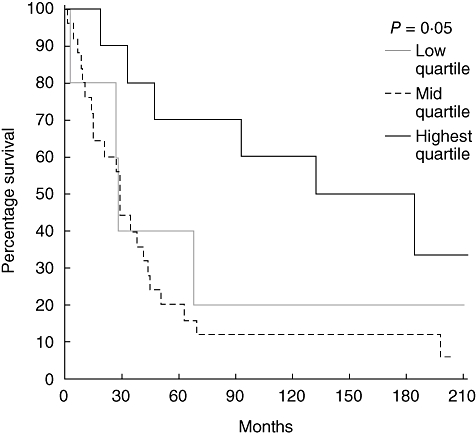
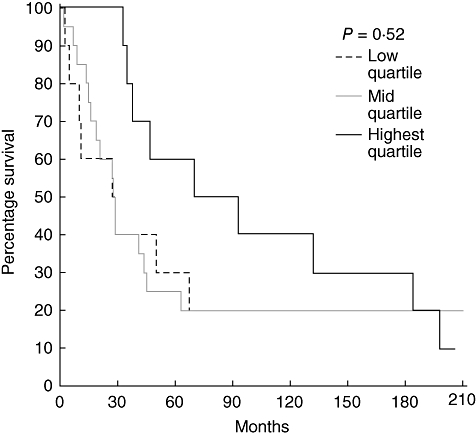
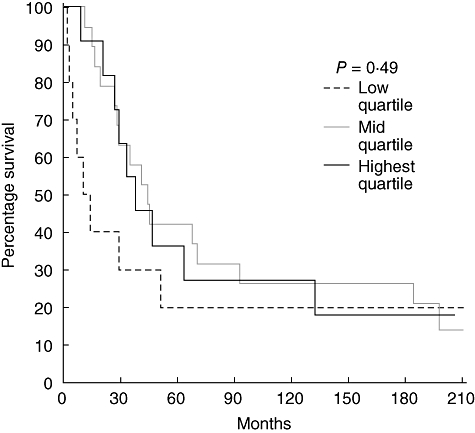
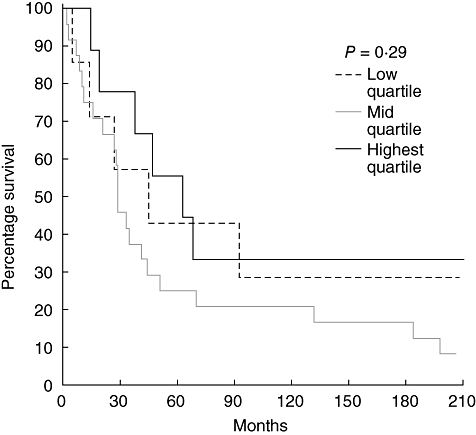
Lymphoid nodules are a normal component of the mucosa of the rectum, but little is known about their function and whether they contribute to the host immune response in malignancy. In rectal cancer specimens from patients with local (n=18), regional (n=12) and distant (n=10) disease, we quantified T cell (CD3, CD25) and dendritic cell (CD1a, CD83) levels at the tumour margin as well as within tumour-associated lymphoid nodules. In normal tissue CD3+, but not CD25+, T cells are concentrated at high levels within lymphoid nodules, with significantly fewer cells found in surrounding normal mucosa (P=0.001). Mature (CD83), but not immature (CD1a), dendritic cells in normal tissue are also found clustered almost exclusively within lymphoid nodules (P=<0.0001). In rectal tumours, both CD3+ T cells (P=0.004) and CD83+ dendritic cells (P=0.0001) are also localized preferentially within tumour-associated lymphoid nodules. However, when comparing tumour specimens to normal rectal tissue, the average density of CD3+ T cells (P=0.0005) and CD83+ dendritic cells (P=0.0006) in tumour-associated lymphoid nodules was significantly less than that seen in lymphoid nodules in normal mucosa. Interestingly, regardless of where quantified, T cell and dendritic cell levels did not depend upon the stage of disease. Increased CD3+ T cell infiltration of tumour-associated lymphoid nodules predicted improved survival, independent of stage (P=0.05). Other T cell (CD25) markers and different levels of CD1a+ or CD83+ dendritic cells did not predict survival. Tumour-associated lymphoid nodules, enriched in dendritic cells and T cells, may be an important site for antigen presentation and increased T cell infiltration may be a marker for improved survival.
Figures
Similar articles
-
Mature dendritic cells make clusters with T cells in the invasive margin of colorectal carcinoma.J Pathol. 2002 Jan;196(1):37-43. doi: 10.1002/path.1018. J Pathol. 2002. PMID: 11748640
-
CD1a- and CD83-positive dendritic cells as prognostic markers of metastasis development in early breast cancer patients.Breast Cancer. 2021 Nov;28(6):1328-1339. doi: 10.1007/s12282-021-01270-9. Epub 2021 Jul 9. Breast Cancer. 2021. PMID: 34240315
-
Prognostic significance of CD83 positive tumor-infiltrating dendritic cells and expression of TGF-beta 1 in human gastric cancer.Hepatogastroenterology. 2011 Sep-Oct;58(110-111):1834-40. doi: 10.5754/hge10320. Hepatogastroenterology. 2011. PMID: 22086706
-
Prognostic value of tumor-infiltrating dendritic cells expressing CD83 in human breast carcinomas.Int J Cancer. 2003 Mar 10;104(1):92-7. doi: 10.1002/ijc.10915. Int J Cancer. 2003. PMID: 12532424
-
Cellular composition of pancreas-associated lymphoid tissue during human fetal pancreatic development.Histopathology. 2004 Sep;45(3):291-7. doi: 10.1111/j.1365-2559.2004.01914.x. Histopathology. 2004. PMID: 15330808
Cited by
-
Tertiary Lymphoid Structures as a Predictive Biomarker of Response to Cancer Immunotherapies.Front Immunol. 2021 May 12;12:674565. doi: 10.3389/fimmu.2021.674565. eCollection 2021. Front Immunol. 2021. PMID: 34054861 Free PMC article. Review.
-
The Crohn's-Like Lymphoid Reaction to Colorectal Cancer-Tertiary Lymphoid Structures With Immunologic and Potentially Therapeutic Relevance in Colorectal Cancer.Front Immunol. 2019 Aug 22;10:1884. doi: 10.3389/fimmu.2019.01884. eCollection 2019. Front Immunol. 2019. PMID: 31507584 Free PMC article. Review.
-
Cancer cell immune mimicry delineates onco-immunologic modulation.iScience. 2021 Sep 15;24(10):103133. doi: 10.1016/j.isci.2021.103133. eCollection 2021 Oct 22. iScience. 2021. PMID: 34632332 Free PMC article.
-
Tumor-infiltrating lymphocyte subsets and tertiary lymphoid structures in pulmonary metastases from colorectal cancer.Clin Exp Metastasis. 2016 Oct;33(7):727-39. doi: 10.1007/s10585-016-9813-y. Epub 2016 Jul 23. Clin Exp Metastasis. 2016. PMID: 27449756 Free PMC article.
-
Neglected no more: B cell-mediated anti-tumor immunity.Semin Immunol. 2023 Jan;65:101707. doi: 10.1016/j.smim.2022.101707. Epub 2022 Dec 15. Semin Immunol. 2023. PMID: 36527759 Free PMC article. Review.
References
-
- Gattaj G, Ciccolallo L. Differences in colorectal cancer survival between European and US populations: the importance of sub-site and morphology. Eur J Cancer. 2003;39:2214–22. - PubMed
-
- Troisi RJ, Freedman AN, Devesa SS. Incidence of colorectal carcinoma in the U.S.: an update of trends by gender, race, age, subsite, and stage, 1975–1994. Cancer. 1999;85:1670–6. - PubMed
-
- Manfredi S, Benhamiche AM, Meny B, et al. Population-based study of factors influencing occurrence and prognosis of local recurrence after surgery for rectal cancer. Br J Surg. 2001;88:1221–7. - PubMed
-
- Rajput A, Bullard Dunn K. Surgical management of rectal cancer. Semin Oncol. 2007;34:241–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
