

Do coder characteristics influence validity of ICD-10 hospital discharge data?
- PMID: 20409320
- PMCID: PMC2868845
- DOI: 10.1186/1472-6963-10-99
Do coder characteristics influence validity of ICD-10 hospital discharge data?
Abstract
Background: Administrative data are widely used to study health systems and make important health policy decisions. Yet little is known about the influence of coder characteristics on administrative data validity in these studies. Our goal was to describe the relationship between several measures of validity in coded hospital discharge data and 1) coders' volume of coding (> or = 13,000 vs. <13,000 records), 2) coders' employment status (full- vs. part-time), and 3) hospital type.
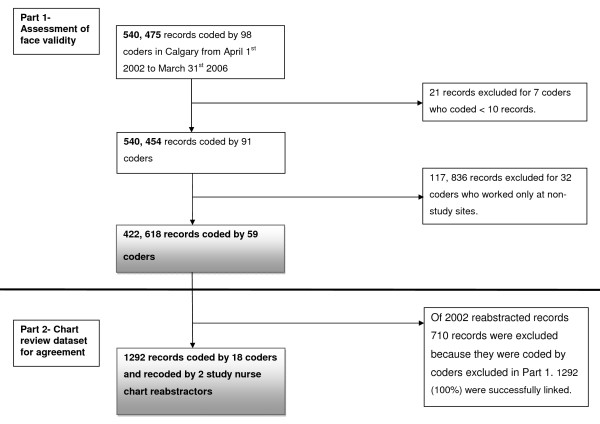
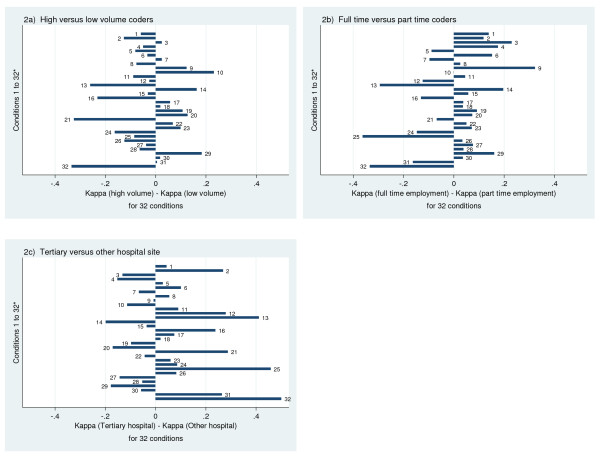
Methods: This descriptive study examined 6 indicators of face validity in ICD-10 coded discharge records from 4 hospitals in Calgary, Canada between April 2002 and March 2007. Specifically, mean number of coded diagnoses, procedures, complications, Z-codes, and codes ending in 8 or 9 were compared by coding volume and employment status, as well as hospital type. The mean number of diagnoses was also compared across coder characteristics for 6 major conditions of varying complexity. Next, kappa statistics were computed to assess agreement between discharge data and linked chart data reabstracted by nursing chart reviewers. Kappas were compared across coder characteristics.
Results: 422,618 discharge records were coded by 59 coders during the study period. The mean number of diagnoses per record decreased from 5.2 in 2002/2003 to 3.9 in 2006/2007, while the number of records coded annually increased from 69,613 to 102,842. Coders at the tertiary hospital coded the most diagnoses (5.0 compared with 3.9 and 3.8 at other sites). There was no variation by coder or site characteristics for any other face validity indicator. The mean number of diagnoses increased from 1.5 to 7.9 with increasing complexity of the major diagnosis, but did not vary with coder characteristics. Agreement (kappa) between coded data and chart review did not show any consistent pattern with respect to coder characteristics.
Conclusions: This large study suggests that coder characteristics do not influence the validity of hospital discharge data. Other jurisdictions might benefit from implementing similar employment programs to ours, e.g.: a requirement for a 2-year college training program, a single management structure across sites, and rotation of coders between sites. Limitations include few coder characteristics available for study due to privacy concerns.
Figures
Similar articles
-
Documentation and coding of ED patient encounters: an evaluation of the accuracy of an electronic medical record.Am J Emerg Med. 2006 Oct;24(6):664-78. doi: 10.1016/j.ajem.2006.02.005. Am J Emerg Med. 2006. PMID: 16984834
-
Reliability measurement and ICD-10 validation of ICPC-2 for coding/classification of diagnoses/health problems in an African primary care setting.Fam Pract. 2018 Jul 23;35(4):406-411. doi: 10.1093/fampra/cmx132. Fam Pract. 2018. PMID: 30060181
-
Improving discharge data fidelity for use in large administrative databases.Neurosurg Focus. 2014 Jun;36(6):E2. doi: 10.3171/2014.3.FOCUS1459. Neurosurg Focus. 2014. PMID: 24881634
-
Administrative data have high variation in validity for recording heart failure.Can J Cardiol. 2010 Oct;26(8):306-12. doi: 10.1016/s0828-282x(10)70438-4. Can J Cardiol. 2010. PMID: 20931099 Free PMC article. Review.
-
Identifying priorities in methodological research using ICD-9-CM and ICD-10 administrative data: report from an international consortium.BMC Health Serv Res. 2006 Jun 15;6:77. doi: 10.1186/1472-6963-6-77. BMC Health Serv Res. 2006. PMID: 16776836 Free PMC article.
Cited by
-
Costs of venous thromboembolism associated with hospitalization for medical illness.Am J Manag Care. 2015 Apr 1;21(4):e255-63. Am J Manag Care. 2015. PMID: 26244788 Free PMC article.
-
Promotion of training course on ICD-10 Poisoning coding : necessity to adopt preventive strategies.BMC Med Educ. 2023 Nov 27;23(1):903. doi: 10.1186/s12909-023-04879-w. BMC Med Educ. 2023. PMID: 38012677 Free PMC article.
-
Coding OSICS sports injury diagnoses in epidemiological studies: does the background of the coder matter?Br J Sports Med. 2014 Apr;48(7):552-6. doi: 10.1136/bjsports-2012-091219. Epub 2012 Aug 23. Br J Sports Med. 2014. PMID: 22919021 Free PMC article.
-
Evaluation of the Effect of Surgeon's Operative Volume and Specialty on Likelihood of Revision After Mesh Midurethral Sling Placement.Obstet Gynecol. 2019 Jun;133(6):1099-1108. doi: 10.1097/AOG.0000000000003275. Obstet Gynecol. 2019. PMID: 31135723 Free PMC article.
-
Visualisation and optimisation of alcohol-related hospital admissions ICD-10 codes in Welsh e-cohort data.Int J Popul Data Sci. 2021 Mar 24;6(1):1373. doi: 10.23889/ijpds.v6i1.1373. Int J Popul Data Sci. 2021. PMID: 34007894 Free PMC article.
References
-
- Iezzoni L. Risk adjustment for measuring health care outcomes. 3. Chicago: Health Administration Press; 2003.
-
- Jurrlink D, Preyra C, Croxford R, Chong A, Austin P, Tu JV. Canadian Institute for Health Information Discharge Abstract Database: A Validation Study. Toronto: Institute for Clinical and Evaluative Sciences; 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
