

Ocular pathology in multiple sclerosis: retinal atrophy and inflammation irrespective of disease duration
- PMID: 20410146
- PMCID: PMC2877904
- DOI: 10.1093/brain/awq080
Ocular pathology in multiple sclerosis: retinal atrophy and inflammation irrespective of disease duration
Abstract
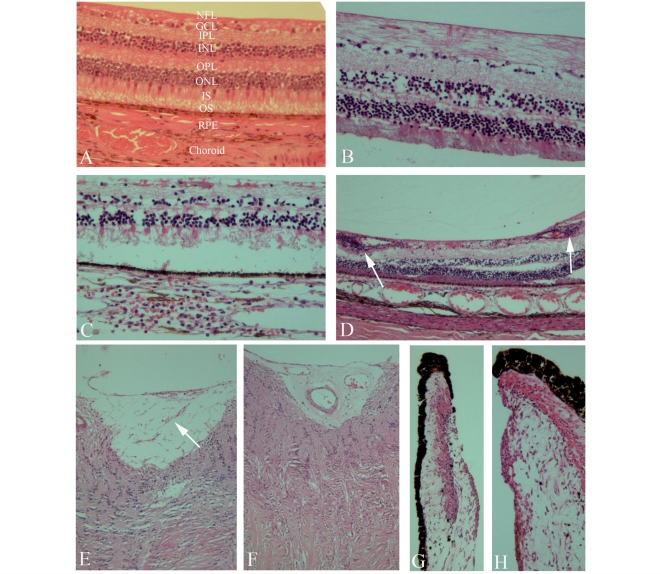
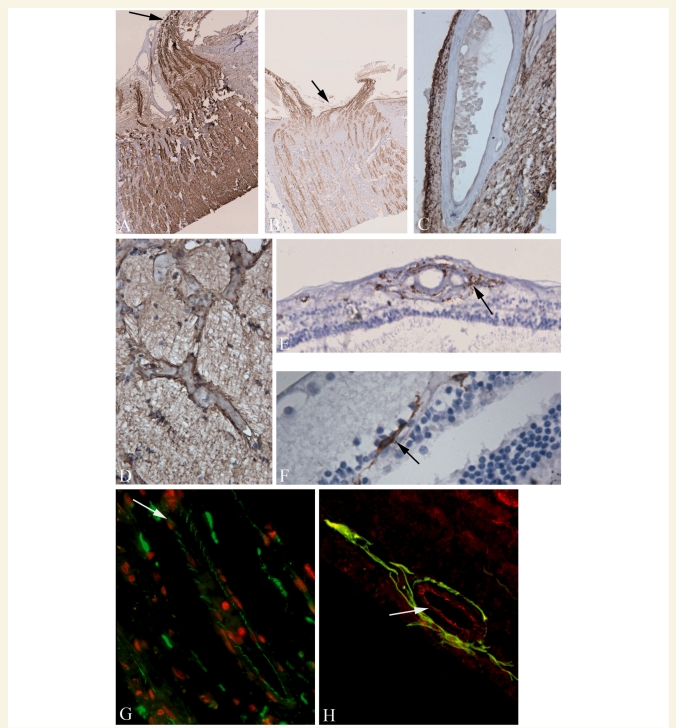
There has been growing interest in the use of retinal imaging for tracking disease progression in multiple sclerosis. However, systematic and detailed pathological descriptions of retinal tissue in multiple sclerosis are lacking. Graded, histological evaluations on eyes from 82 patients with multiple sclerosis and 10 subjects with other neurological diseases, with immunohistochemistry on a subset, were performed and correlated with clinical and pathological findings. Multiple sclerosis cases demonstrated evidence of retinal atrophy and inflammation even in late-stage disease. Retinal ganglion cell loss was significant and remaining neurons appeared shrunken and were partially engulfed by human leukocyte antigen-DR positive cells with the phenotype of microglia in samples subjected to immunohistochemistry. Neurofilament staining revealed variable but prominent degrees of axonal loss and injury. Neuronal loss was noted in the inner nuclear layer with focal reduction in cell density. Foamy-appearing human leukocyte antigen-DR positive cells were evident near vessels and periphlebitis was found in a small but significant number of multiple sclerosis cases. Glial fibrillary acidic protein staining showed extensive astrocyte hypertrophy and proliferation with prominent gliosis in multiple sclerosis cases. Frequent but previously unreported abnormalities in the iris were documented in the majority of chronic multiple sclerosis cases. The injury to both iris and retina could be seen at all stages of disease. Severity of retinal atrophy was correlated with overall brain weight at time of autopsy (P = 0.04) and a trend for increased atrophy was seen with longer disease duration (P = 0.13). This study provides the first large-scale pathological description of retinas in multiple sclerosis, including patients with different subtypes of disease at all stages, and with variable clinical severity. Changes were seen not only in the retinal nerve fibre layer and ganglion cell layer, but also in the inner nuclear layer, suggesting that retinal injury is more widespread than previously appreciated. Furthermore, the human retina is devoid of myelin, but inflammation was demonstrated to be prominent in multiple sclerosis and to persist in the retina at late stages of disease. The prominent gliosis and inflammation surrounding vessels of the inner retina could potentially impact optical coherence tomography evaluations in multiple sclerosis-as standard techniques exploit presumed differences in tissue reflectivity and utilize automated edge detection algorithms to judge axon loss in the nerve fibre layer. Deciphering the relationships between the different types of retinal pathology may aid us in understanding the factors that drive both inflammation and tissue atrophy in multiple sclerosis.
Figures
References
-
- Arnold C. Evolving management of optic neuritis and multiple sclerosis. J Ophthalmol. 2005;139:1101–108. - PubMed
-
- Arnold AC, Pepose JS, Hepler RS, Foos RY. Retinal periphlebitis and retinitis in multiple sclerosis. I. Pathologic characteristics. Ophthalmology. 1984;91:255–62. - PubMed
-
- Balcer LJ. Optic Neuritis. N Engl J Med. 2006;354:1273–80. - PubMed
-
- Birch MK, Barbosa S, Blumhardt LD, O'Brien C, Harding SP. Retinal venous sheathing and the blood-retinal barrier in multiple sclerosis. Arch Ophthalmol. 1996;114:34–9. - PubMed
-
- Biousse V, Trichet C, Bloch-Michel E, Roullet E. Multiple sclerosis associated with uveitis in two large clinic-based series. Neurology. 1999;52:179–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
