

Prevalence of congenital heart defects and persistent pulmonary hypertension of the neonate with Down syndrome
- PMID: 20411274
- PMCID: PMC2926442
- DOI: 10.1007/s00431-010-1200-0
Prevalence of congenital heart defects and persistent pulmonary hypertension of the neonate with Down syndrome
Abstract
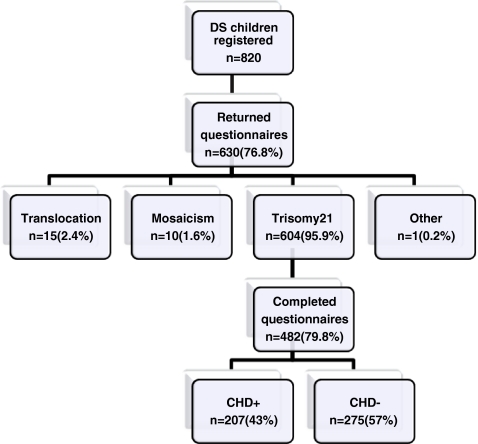
The aim of this study was to assess the prevalence of congenital heart defects (CHDs) and persistent pulmonary hypertension of the neonate (PPHN) in children with Down syndrome (DS) and to assess its impact on neonatal factors. It was a prospective study of a birth cohort of children with DS born between 2003 and 2006 registered by the Dutch Paediatric Surveillance Unit (DPSU). A CHD occurred in 43% of 482 children with trisomy 21. Atrioventricular septal defect was found in 54%, ventricular septal defect in 33.3% and patent ductus arteriosus in 5.8%. The incidence of PPHN in DS was 5.2%, which is significantly higher than the general population (p < 0.001). The reported mortality in newborns with DS was overall 3.3% and was still significant higher in children with a CHD versus no CHD (5.8% versus 1.5%) (p = 0.008). The presence of CHD in children with DS had no influence on their birth weight, mean gestational age and Apgar score. In neonates with DS, we found not only a 43% prevalence of CHD, but also a high incidence of PPHN at 5.2%. Early recognition of the cardiac condition of neonates with DS seems justified.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
