

Three pathways for human kidney stone formation
- PMID: 20411383
- PMCID: PMC3169174
- DOI: 10.1007/s00240-010-0271-8
Three pathways for human kidney stone formation
Abstract
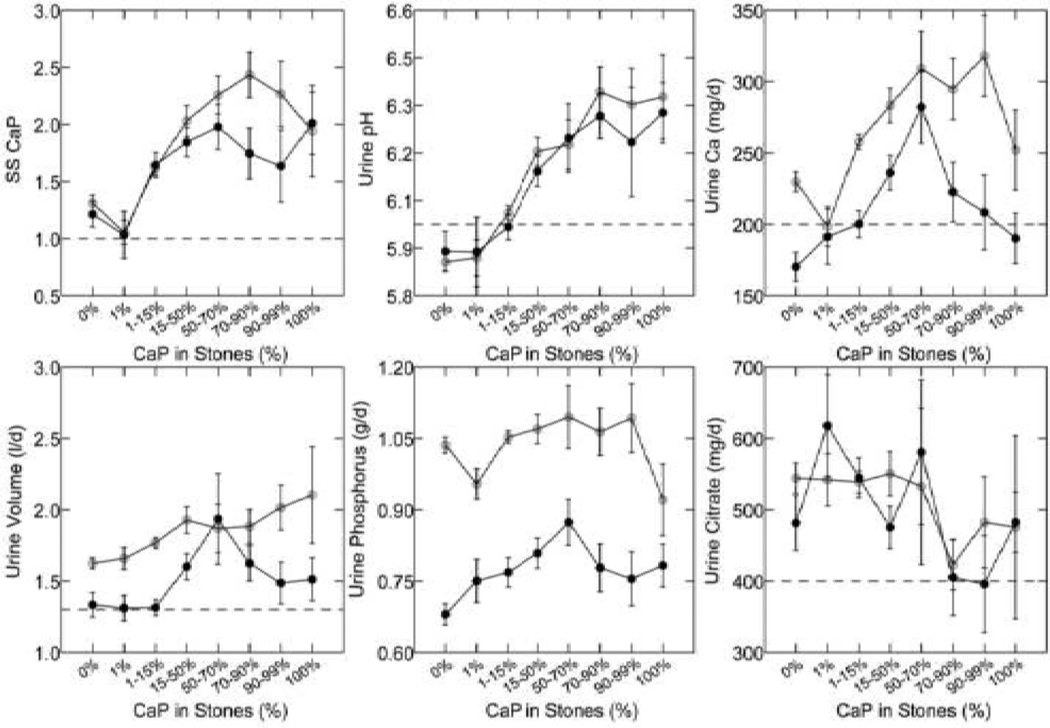
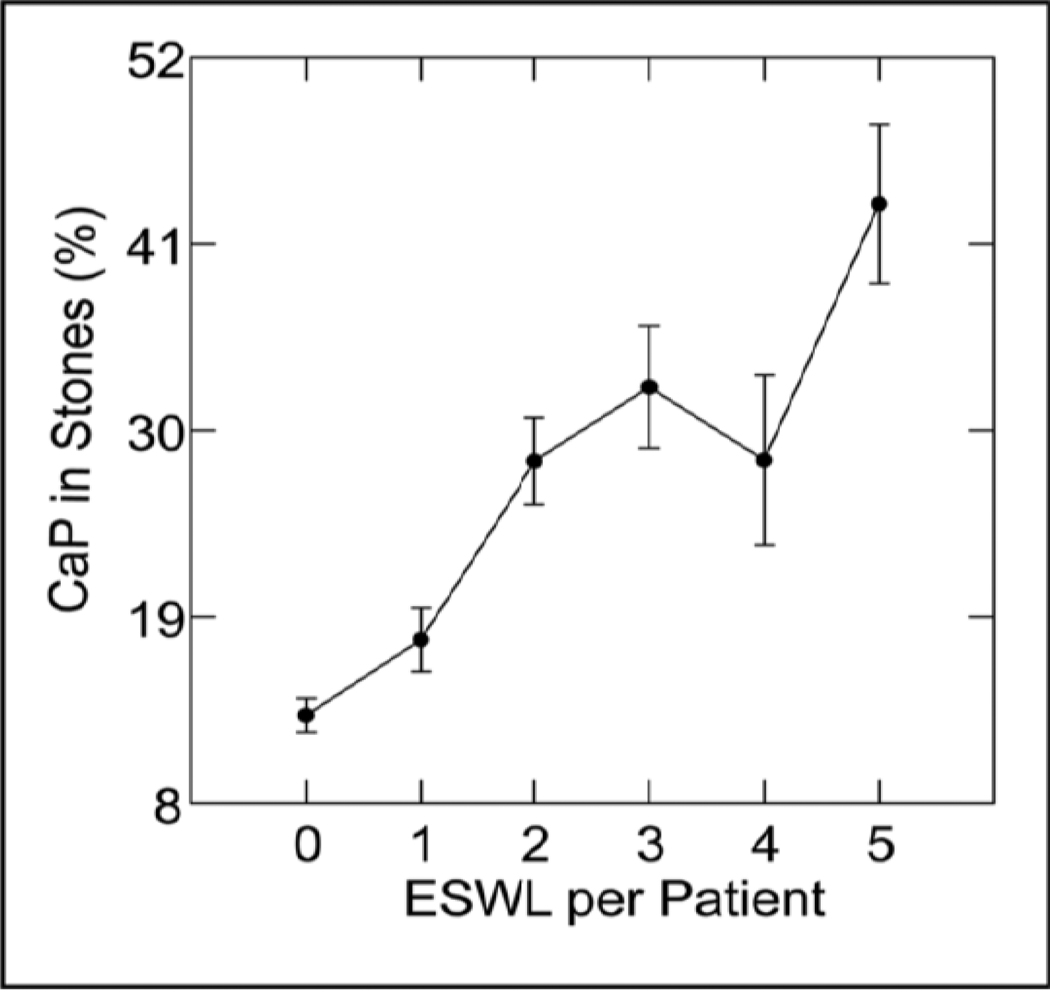
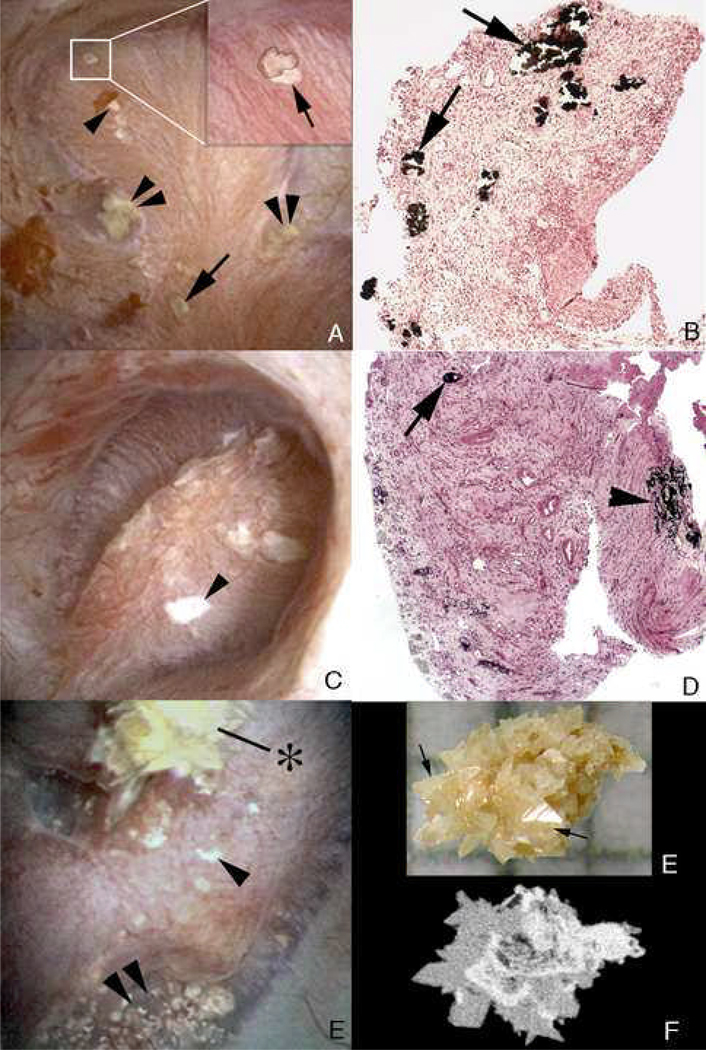
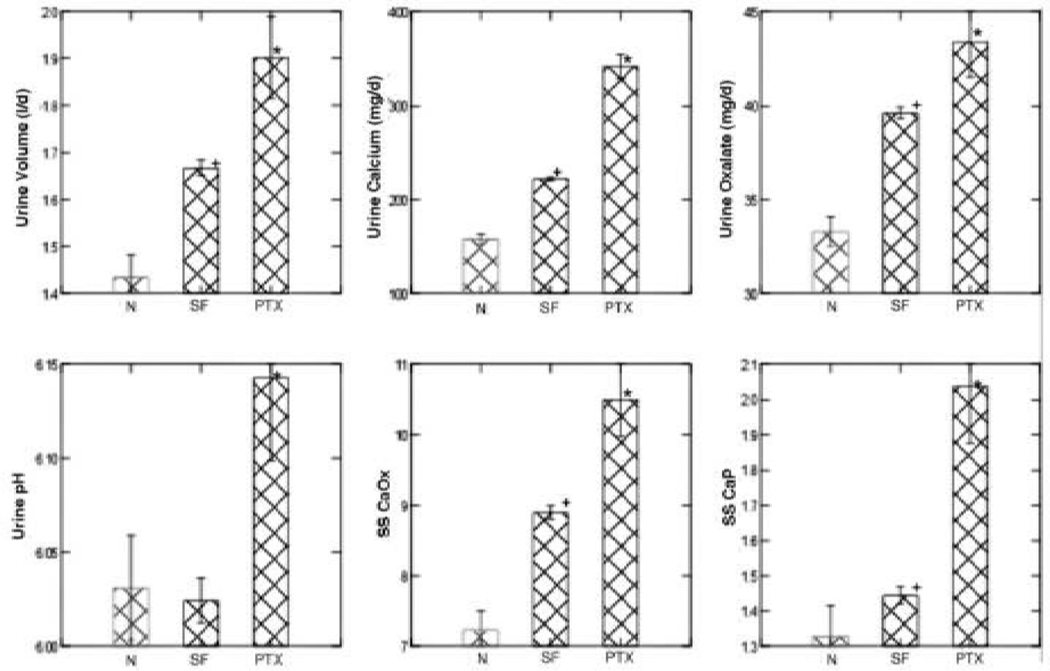
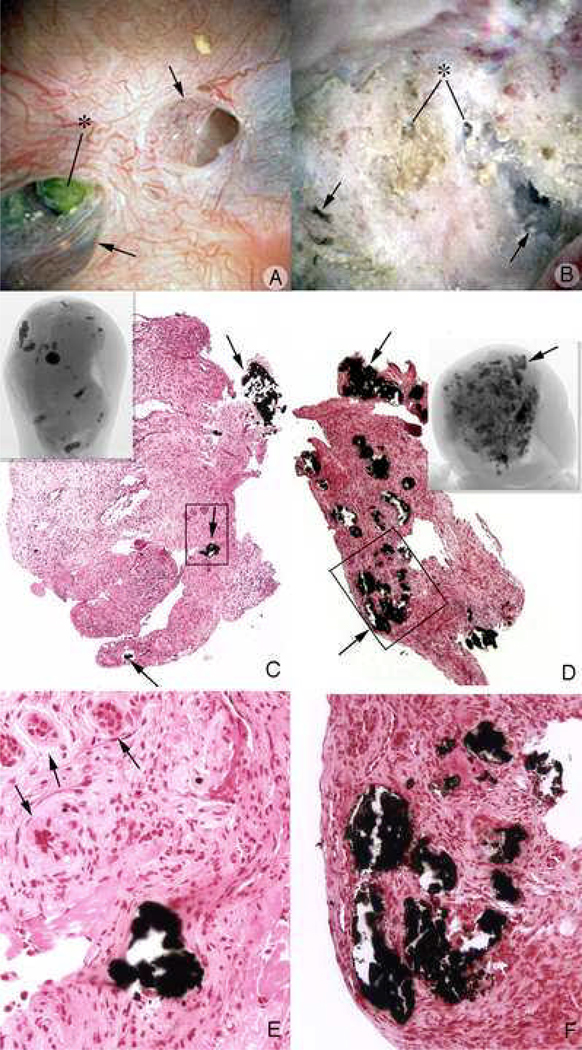
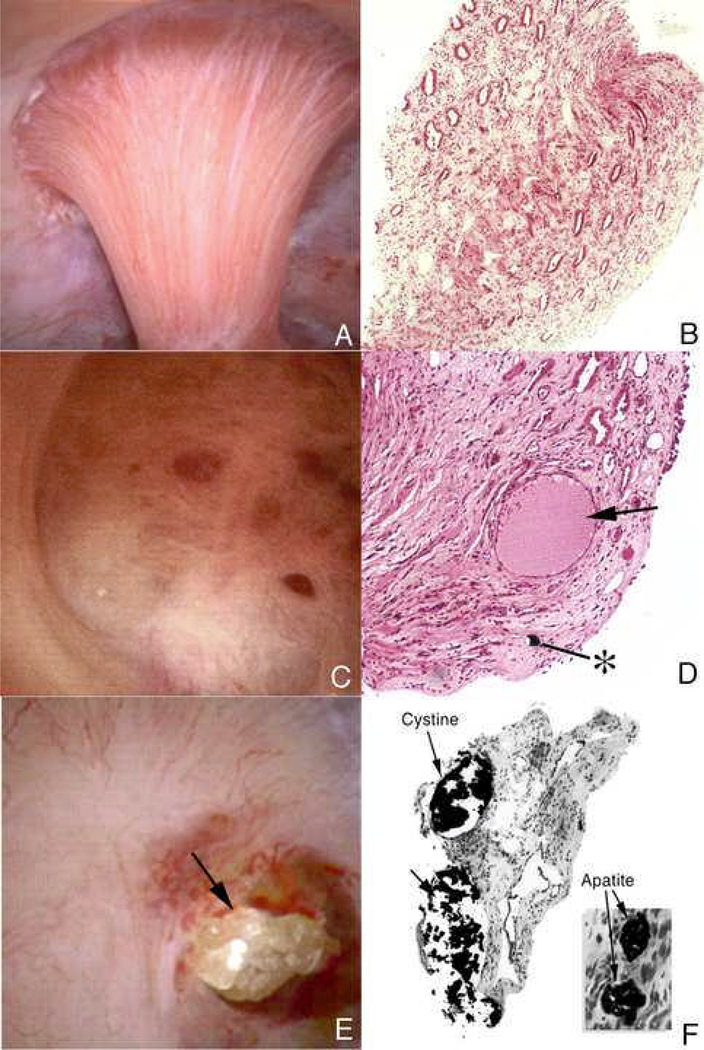
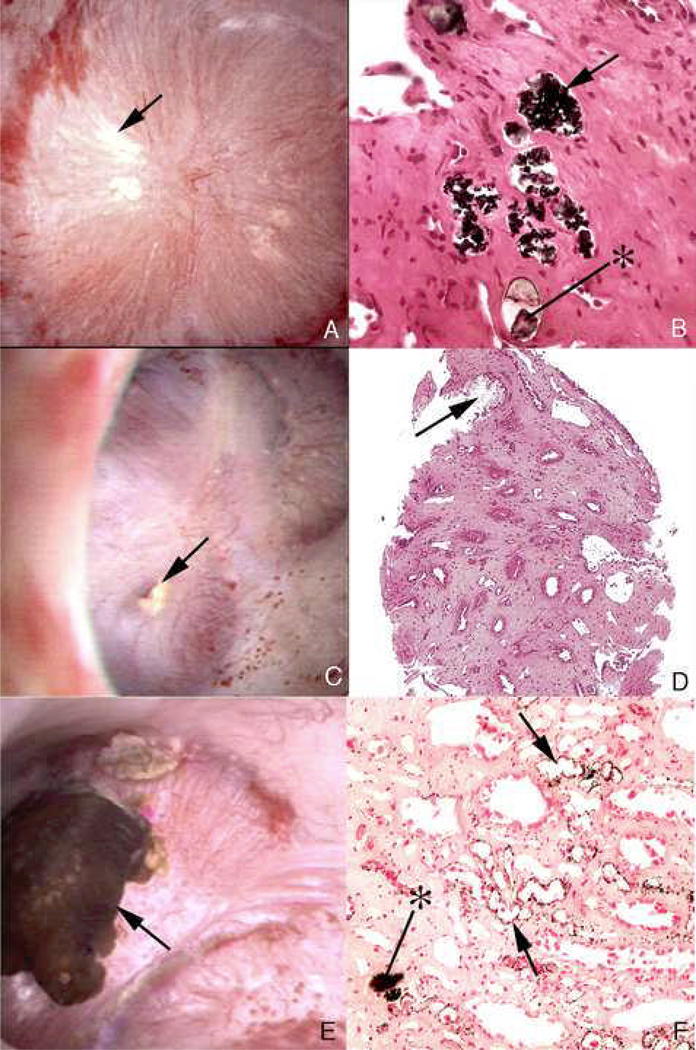
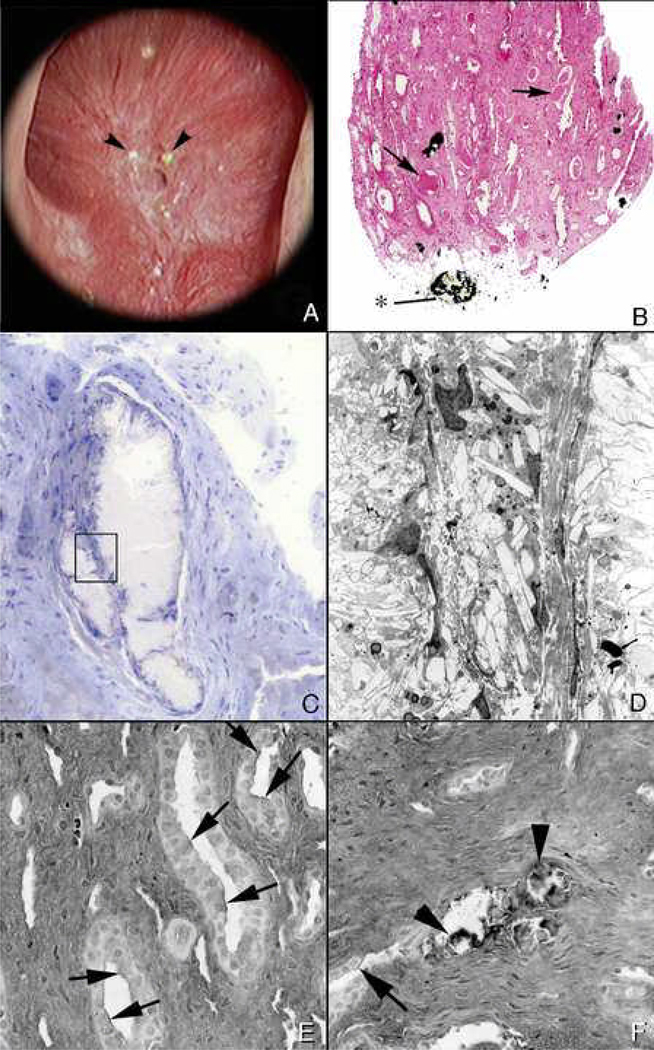
No single theory of pathogenesis can properly account for human kidney stones, they are too various and their formation is too complex for simple understanding. Using human tissue biopsies, intraoperative imaging and such physiology data from ten different stone forming groups, we have identified at least three pathways that lead to stones. The first pathway is overgrowth on interstitial apatite plaque as seen in idiopathic calcium oxalate stone formers, as well as stone formers with primary hyperparathyroidism, ileostomy, and small bowel resection, and in brushite stone formers. In the second pathway, there are crystal deposits in renal tubules that were seen in all stone forming groups except the idiopathic calcium oxalate stone formers. The third pathway is free solution crystallization. Clear examples of this pathway are those patient groups with cystinuria or hyperoxaluria associated with bypass surgery for obesity. Although the final products may be very similar, the ways of creation are so different that in attempting to create animal and cell models of the processes one needs to be careful that the details of the human condition are included.
Figures
References
-
- Evan A, Lingeman J, Coe FL, Worcester E. Randall's plaque: pathogenesis and role in calcium oxalate nephrolithiasis. Kidney Int. 2006;69:1313–1318. - PubMed
-
- Matlaga BR, Williams JC, Jr, Kim SC, Kuo RL, Evan AP, Bledsoe SB, Coe FL, Worcester EM, Munch LC, Lingeman JE. Endoscopic evidence of calculus attachment to Randall's plaque. J Urol. 2006;175:1720–1724. - PubMed
-
- Randall R. Papillary pathology as precursor of primary renal calculus. Journal of Urology. 1940;44:580–589.
-
- Evan AP, Coe FL, Rittling SR, Bledsoe SM, Shao Y, Lingeman JE, Worcester EM. Apatite plaque particles in inner medulla of kidneys of calcium oxalate stone formers: osteopontin localization. Kidney Int. 2005;68:145–154. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
