

Obesity does not preclude safe and effective myeloablative hematopoietic cell transplantation (HCT) for acute myelogenous leukemia (AML) in adults
- PMID: 20412867
- PMCID: PMC2933950
- DOI: 10.1016/j.bbmt.2010.04.009
Obesity does not preclude safe and effective myeloablative hematopoietic cell transplantation (HCT) for acute myelogenous leukemia (AML) in adults
Abstract
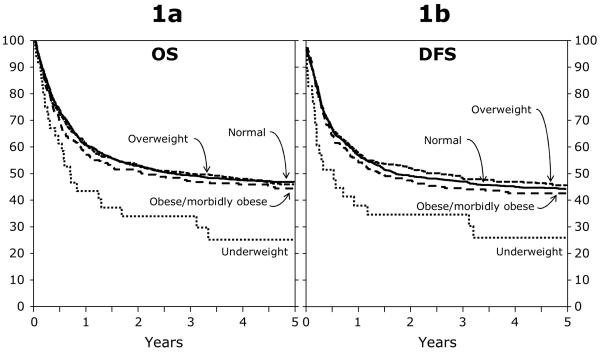
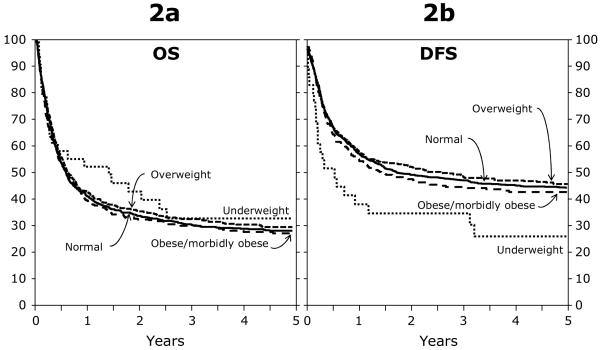
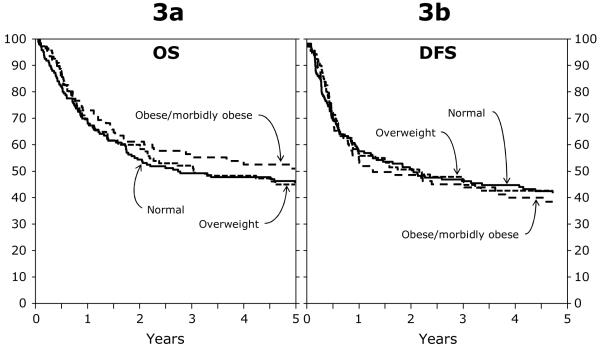
The incidence of excessive adiposity is increasing worldwide, and is associated with numerous adverse health outcomes. We compared outcomes by body mass index (BMI) for adult patients with acute myelogenous leukemia (AML) who underwent autologous (auto, n = 373), related donor (RD, n = 2041), or unrelated donor (URD, n = 1801) allogeneic myeloablative hematopoietic cell transplantation (HCT) using bone marrow or peripheral blood stem cells reported to the Center for International Blood and Marrow Transplant Research (CIBMTR) from 1995 to 2004. Four weight groups by BMI (kg/m(2)) were defined: underweight <18 kg/m(2); normal 18-25 kg/m(2); overweight >25-30 kg/m(2); and obese >30 kg/m(2). Multivariable analysis referenced to the normal weight group showed an increased risk of death for underweight patients in the RD group (relative risk [RR], 1.92; 95% confidence interval [CI], 1.28-2.89; P = .002), but not in the URD group. There were no other differences in outcomes among the other weight groups within the other HCT groups. Overweight and obese patients enjoyed a modest decrease in relapse incidence, although this did not translate into a survival benefit. Small numbers of patients limit the ability to better characterize the adverse outcomes seen in the underweight RD but not the underweight URD allogeneic HCT patients. Obesity alone should not be considered a barrier to HCT.
Copyright © 2010 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Al Rashdan IR, Nesef YA. Prevalance of Overweight, Obesity, and Metabolic Syndrome Among Adult Kuwaitis: Results From Community-based National Survey. Angiology. 2009 - PubMed
-
- Chen CM. Overview of obesity in Mainland China. Obes Rev. 2008;9(Suppl 1):14–21. - PubMed
-
- Kosti RI, Panagiotakos DB. The epidemic of obesity in children and adolescents in the world. Cent Eur J Public Health. 2006;14:151–159. - PubMed
-
- Low S, Chin MC, Deurenberg-Yap M. Review on epidemic of obesity. Ann Acad Med Singapore. 2009;38:57–59. - PubMed
-
- Misra A, Khurana L. Obesity and the metabolic syndrome in developing countries. J Clin Endocrinol Metab. 2008;93:S9–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
