

Muscle metaboreflex-induced coronary vasoconstriction functionally limits increases in ventricular contractility
- PMID: 20413426
- PMCID: PMC2928591
- DOI: 10.1152/japplphysiol.01243.2009
Muscle metaboreflex-induced coronary vasoconstriction functionally limits increases in ventricular contractility
Abstract
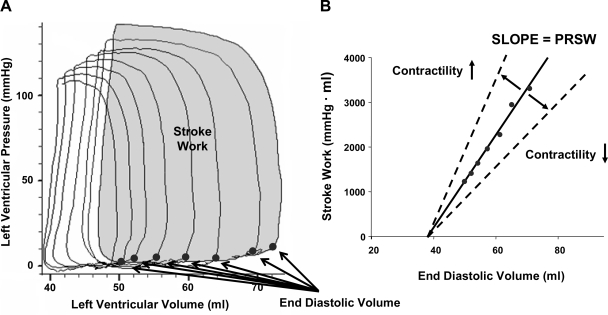
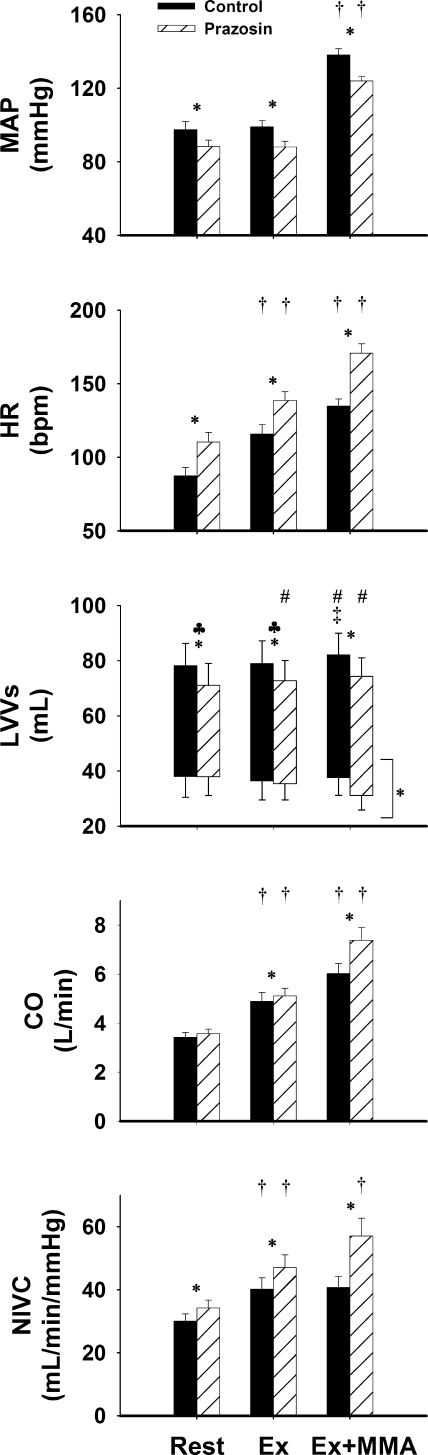
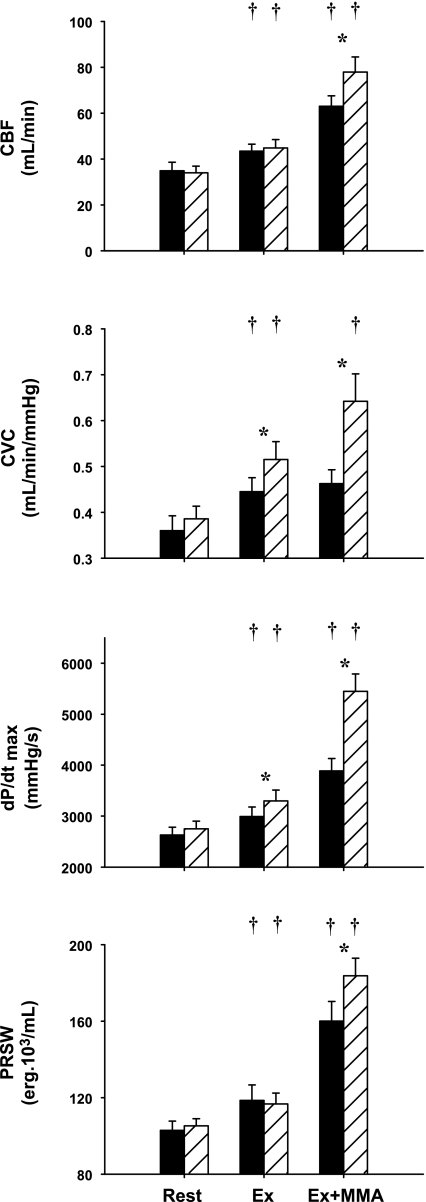
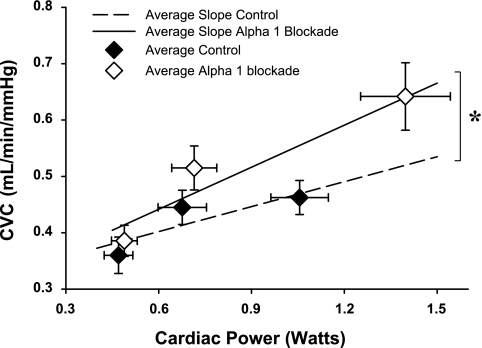
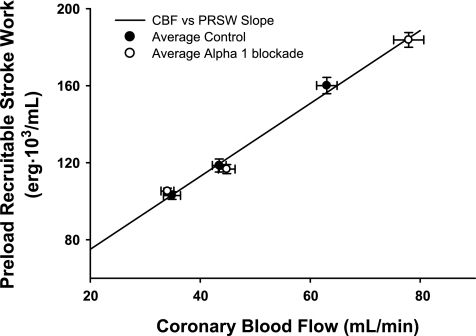
Muscle metaboreflex activation during dynamic exercise induces a substantial increase in cardiac work and oxygen demand via a significant increase in heart rate, ventricular contractility, and afterload. This increase in cardiac work should cause coronary metabolic vasodilation. However, little if any coronary vasodilation is observed due to concomitant sympathetically induced coronary vasoconstriction. The purpose of the present study is to determine whether the restraint of coronary vasodilation functionally limits increases in left ventricular contractility. Using chronically instrumented, conscious dogs (n = 9), we measured mean arterial pressure, cardiac output, and circumflex blood flow and calculated coronary vascular conductance, maximal derivative of ventricular pressure (dp/dt(max)), and preload recruitable stroke work (PRSW) at rest and during mild exercise (2 mph) before and during activation of the muscle metaboreflex. Experiments were repeated after systemic alpha(1)-adrenergic blockade ( approximately 50 microg/kg prazosin). During prazosin administration, we observed significantly greater increases in coronary vascular conductance (0.64 + or - 0.06 vs. 0.46 + or - 0.03 ml x min(-1) x mmHg(-1); P < 0.05), circumflex blood flow (77.9 + or - 6.6 vs. 63.0 + or - 4.5 ml/min; P < 0.05), cardiac output (7.38 + or - 0.52 vs. 6.02 + or - 0.42 l/min; P < 0.05), dP/dt(max) (5,449 + or - 339 vs. 3,888 + or - 243 mmHg/s; P < 0.05), and PRSW (160.1 + or - 10.3 vs. 183.8 + or - 9.2 erg.10(3)/ml; P < 0.05) with metaboreflex activation vs. those seen in control experiments. We conclude that the sympathetic restraint of coronary vasodilation functionally limits further reflex increases in left ventricular contractility.
Figures
Comment in
-
The muscle metaboreflex: reining in the heart?J Appl Physiol (1985). 2010 Aug;109(2):263-4. doi: 10.1152/japplphysiol.00547.2010. Epub 2010 Jun 3. J Appl Physiol (1985). 2010. PMID: 20522736 No abstract available.
Similar articles
-
Exaggerated coronary vasoconstriction limits muscle metaboreflex-induced increases in ventricular performance in hypertension.Am J Physiol Heart Circ Physiol. 2017 Jan 1;312(1):H68-H79. doi: 10.1152/ajpheart.00417.2016. Epub 2016 Oct 21. Am J Physiol Heart Circ Physiol. 2017. PMID: 27769997 Free PMC article.
-
Muscle metaboreflex-induced increases in cardiac sympathetic activity vasoconstrict the coronary vasculature.J Appl Physiol (1985). 2007 Jul;103(1):190-4. doi: 10.1152/japplphysiol.00139.2007. Epub 2007 May 3. J Appl Physiol (1985). 2007. PMID: 17478607
-
Muscle metaboreflex-induced coronary vasoconstriction limits ventricular contractility during dynamic exercise in heart failure.Am J Physiol Heart Circ Physiol. 2013 Apr 1;304(7):H1029-37. doi: 10.1152/ajpheart.00879.2012. Epub 2013 Jan 25. Am J Physiol Heart Circ Physiol. 2013. PMID: 23355344 Free PMC article.
-
Muscle metaboreflex control of the circulation during exercise.Acta Physiol (Oxf). 2010 Aug;199(4):367-83. doi: 10.1111/j.1748-1716.2010.02133.x. Epub 2010 Mar 27. Acta Physiol (Oxf). 2010. PMID: 20353495 Review.
-
Altered reflex cardiovascular control during exercise in heart failure: animal studies.Exp Physiol. 2006 Jan;91(1):73-7. doi: 10.1113/expphysiol.2005.031179. Epub 2005 Sep 22. Exp Physiol. 2006. PMID: 16179406 Review.
Cited by
-
Role of cardiac output versus peripheral vasoconstriction in mediating muscle metaboreflex pressor responses: dynamic exercise versus postexercise muscle ischemia.Am J Physiol Regul Integr Comp Physiol. 2013 Apr 15;304(8):R657-63. doi: 10.1152/ajpregu.00601.2012. Epub 2013 Feb 20. Am J Physiol Regul Integr Comp Physiol. 2013. PMID: 23427084 Free PMC article.
-
Augmented sympathoexcitation slows postexercise heart rate recovery.J Appl Physiol (1985). 2023 Dec 1;135(6):1300-1311. doi: 10.1152/japplphysiol.00549.2023. Epub 2023 Oct 26. J Appl Physiol (1985). 2023. PMID: 37883101 Free PMC article.
-
Muscle metaboreflex activation during dynamic exercise evokes epinephrine release resulting in β2-mediated vasodilation.Am J Physiol Heart Circ Physiol. 2015 Mar 1;308(5):H524-9. doi: 10.1152/ajpheart.00648.2014. Epub 2014 Dec 24. Am J Physiol Heart Circ Physiol. 2015. PMID: 25539712 Free PMC article.
-
Exaggerated coronary vasoconstriction limits muscle metaboreflex-induced increases in ventricular performance in hypertension.Am J Physiol Heart Circ Physiol. 2017 Jan 1;312(1):H68-H79. doi: 10.1152/ajpheart.00417.2016. Epub 2016 Oct 21. Am J Physiol Heart Circ Physiol. 2017. PMID: 27769997 Free PMC article.
-
Arterial Baroreflex Inhibits Muscle Metaboreflex Induced Increases in Effective Arterial Elastance: Implications for Ventricular-Vascular Coupling.Front Physiol. 2022 Mar 25;13:841076. doi: 10.3389/fphys.2022.841076. eCollection 2022. Front Physiol. 2022. PMID: 35399256 Free PMC article.
References
-
- Ansorge EJ, Augustyniak RA, Perinot RL, Hammond RL, Kim JK, Sala-Mercado JA, Rodriguez J, Rossi NF, O'Leary DS. Altered muscle metaboreflex control of coronary blood flow and ventricular function in heart failure. Am J Physiol Heart Circ Physiol 288: H1381–H1388, 2005 - PubMed
-
- Ansorge EJ, Shah SH, Augustyniak R, Rossi NF, Collins HL, O'Leary DS. Muscle metaboreflex control of coronary blood flow. Am J Physiol Heart Circ Physiol 283: H526–H532, 2002 - PubMed
-
- Asmussen E, Nielsen M. Experiments on nervous factors controlling respiration and circulation during exercise employing blocking of the blood flow. Acta Physiol Scand 60: 103–111, 1964 - PubMed
-
- Augustyniak RA, Ansorge EJ, O'Leary DS. Muscle metaboreflex control of cardiac output and peripheral vasoconstriction exhibit differential latencies. Am J Physiol Heart Circ Physiol 278: H530–H537, 2000 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous