

Clinical and genetic spectrum of Birt-Hogg-Dube syndrome patients in whom pneumothorax and/or multiple lung cysts are the presenting feature
- PMID: 20413710
- PMCID: PMC2981024
- DOI: 10.1136/jmg.2009.070565
Clinical and genetic spectrum of Birt-Hogg-Dube syndrome patients in whom pneumothorax and/or multiple lung cysts are the presenting feature
Abstract
Background: Birt-Hogg-Dubé syndrome (BHDS) is an inherited autosomal genodermatosis characterised by fibrofolliculomas of the skin, renal tumours and multiple lung cysts. Genetic studies have disclosed that the clinical picture as well as responsible germline FLCN mutations are diverse.
Objectives: BHDS may be caused by a germline deletion which cannot be detected by a conventional genetic approach. Real-time quantitative polymerase chain reaction (qPCR) may be able to identify such a mutation and thus provide us with a more accurate clinical picture of BHDS.
Methods: This study analysed 36 patients with multiple lung cysts of undetermined causes. Denaturing high performance liquid chromatography (DHPLC) was applied for mutation screening. If no abnormality was detected by DHPLC, the amount of each FLCN exon in genome was quantified by qPCR.
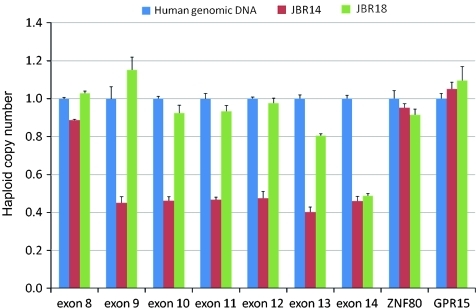
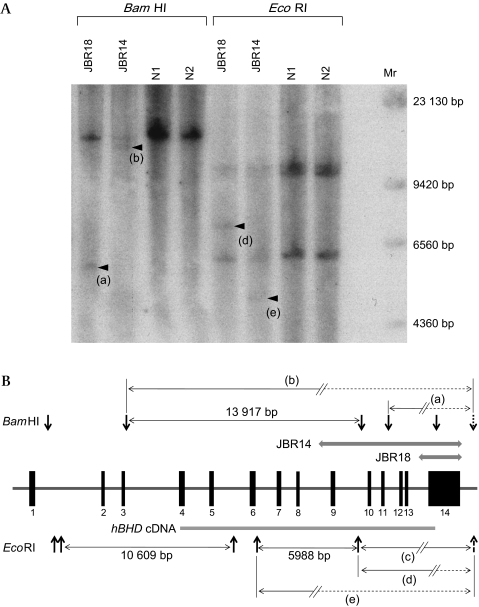
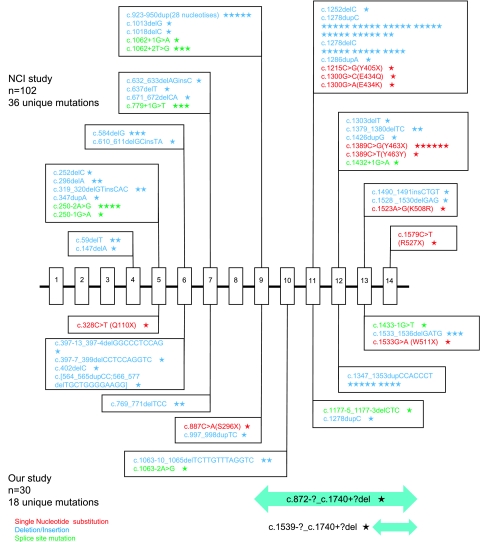
Results: An FLCN germline mutation was found in 23 (63.9%) of the 36 patients by DHPLC and direct sequencing (13 unique small nucleotide alterations which included 11 novel mutations). A large genomic deletion was identified in two of the remaining 13 patients by qPCR (one patient with exon 14 deletion and one patient with a deletion encompassing exons 9 to 14). Mutations including genomic deletions were most frequently identified in the 3'-end of the FLCN gene including exons 12 and 13 (13/25=52.0%). The BHDS patients whose multiple cysts prompted the diagnosis in this study showed a very low incidence of skin and renal involvement.
Conclusions: BHDS is due to large deletions as well as small nucleotide alterations. Racial differences may occur between Japanese and patients of European decent in terms of FLCN mutations and clinical manifestations.
Conflict of interest statement
Figures
References
-
- Birt AR, Hogg GR, Dube WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol 1977;113:1674–7 - PubMed
-
- Vincent A, Farley M, Chan E, et al. Birt-Hogg-Dube syndrome: a review of the literature and the differential diagnosis of firm facial papules. J Am Acad Dermatol 2003;49:698–705 - PubMed
-
- Roth JS, Rabinowitz AD, Benson M, et al. Bilateral renal cell carcinoma in the Birt-Hogg-Dube syndrome. J Am Acad Dermatol 1993;29:1055–6 - PubMed
-
- Toro JR, Glenn G, Duray P, et al. Birt-Hogg-Dube syndrome: a novel marker of kidney neoplasia. Arch Dermatol 1999;135:1195–202 - PubMed
-
- Binet O, Audefray D, Beltzer-Garelly E, et al. [Haber's syndrome. First French family (2 cases)]. Ann Dermatol Venereol 1986;113:43–50 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases