

Acetabular cartilage thickness: accuracy of three-dimensional reconstructions from multidetector CT arthrograms in a cadaver study
- PMID: 20413764
- PMCID: PMC2858813
- DOI: 10.1148/radiol.10081876
Acetabular cartilage thickness: accuracy of three-dimensional reconstructions from multidetector CT arthrograms in a cadaver study
Abstract
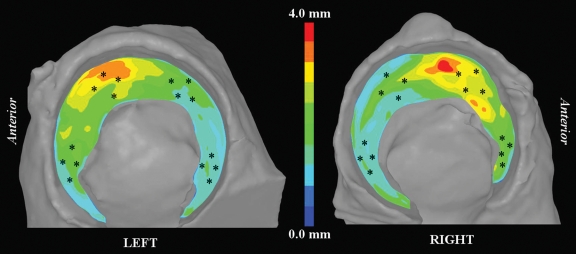
Purpose: To prospectively quantify the accuracy of hip cartilage thickness estimated from three-dimensional (3D) surfaces, generated by segmenting multidetector computed tomographic (CT) arthrograms by using direct physical measurements of cartilage thickness as the reference standard.
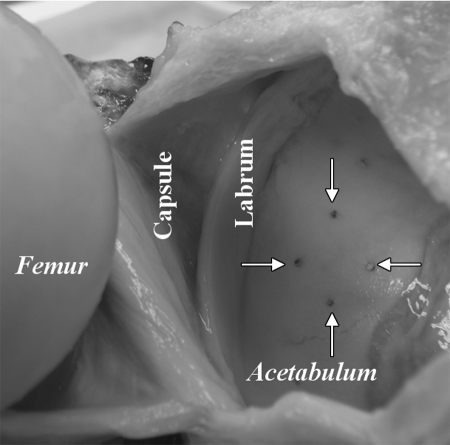
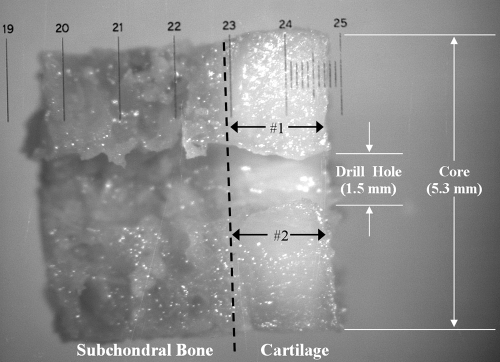
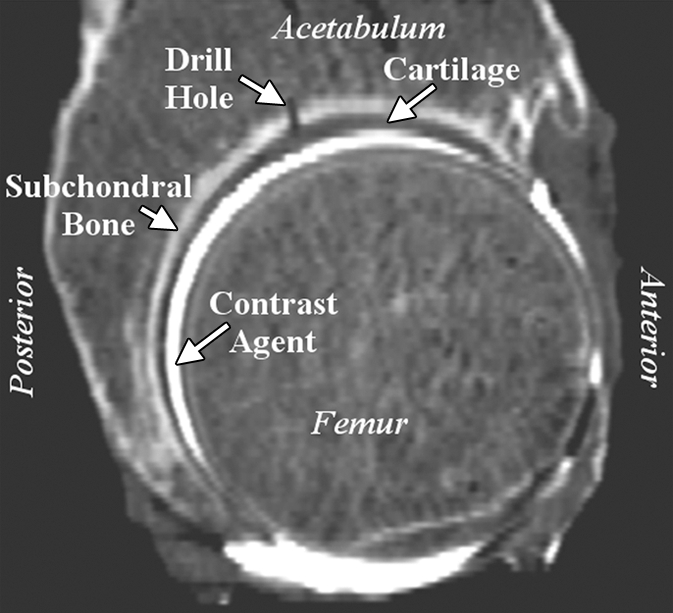
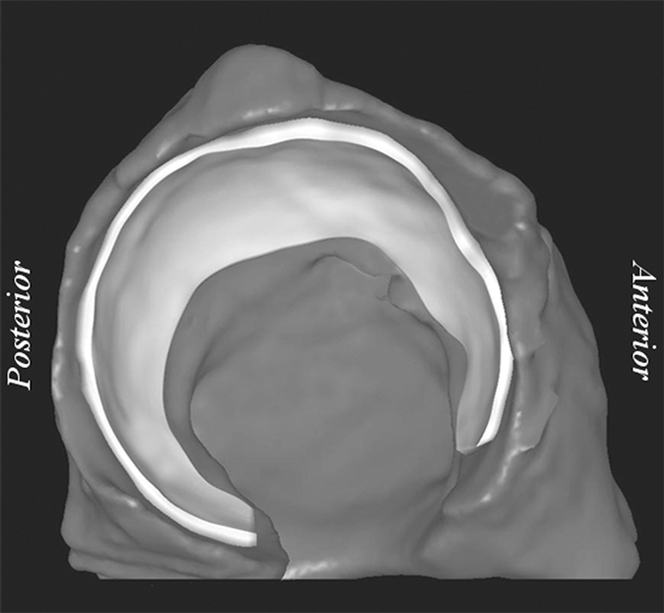
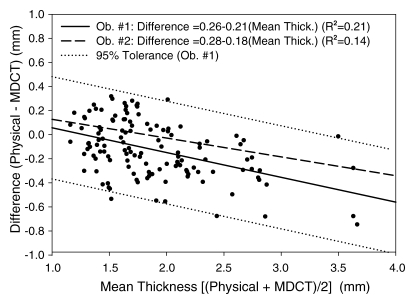
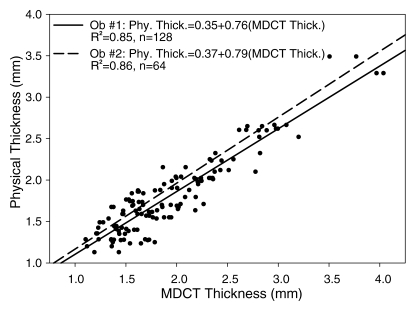
Materials and methods: Four fresh-frozen cadaver hip joints from two male donors, ages 43 and 46 years, were obtained; institutional review board approval for cadaver research was also obtained. Sixteen holes were drilled perpendicular to the cartilage of four cadaveric acetabula (two specimens). Hip capsules were surgically closed, injected with contrast material, and scanned by using multidetector CT. After scanning, 5.3-mmcores were harvested concentrically at each drill hole and cartilage thickness was measured with a microscope. Cartilage was reconstructed in 3D by using commercial software. Segmentations were repeated by two authors. Reconstructed cartilage thickness was determined by using a published algorithm. Bland-Altman plots and linear regression were used to assess accuracy. Repeatability was quantified by using the coefficient of variation, intraclass correlation coefficient (ICC), repeatability coefficient, and percentage variability.
Results: Cartilage was reconstructed to a bias of -0.13 mm and a repeatability coefficient of + or - 0.46 mm. Regression of the scatterplots indicated a tendency for multidetector CT to overestimate thickness. Intra- and interobserver repeatability were very good. For intraobserver correlation, the coefficient of variation was 14.80%, the ICC was 0.88, the repeatability coefficient was 0.55 mm, and the percentage variability was 11.77%. For interobserver correlation, the coefficient of variation was 13.47%, the ICC was 0.90, the repeatability coefficient was 0.52 mm, and the percentage variability was 11.63%.
Conclusion: Assuming that an accuracy of approximately + or - 0.5 mm is sufficient, reconstructions of cartilage geometry from multidetector CT arthrographic data could be used as a preoperative surgical planning tool.
Figures
References
-
- Nishii T, Sugano N, Tanaka H, Nakanishi K, Ohzono K, Yoshikawa H. Articular cartilage abnormalities in dysplastic hips without joint space narrowing. Clin Orthop Relat Res 2001;(383):183–190 - PubMed
-
- Nishii T, Tanaka H, Nakanishi K, Sugano N, Miki H, Yoshikawa H. Fat-suppressed 3D spoiled gradient-echo MRI and MDCT arthrography of articular cartilage in patients with hip dysplasia. AJR Am J Roentgenol 2005;185(2):379–385 - PubMed
-
- Tönnis D.Congenital dysplasia and dislocation of the hip in children and adults Berlin, Germany: Springer-Verlag, 1987
-
- Mechlenburg I.Evaluation of Bernese periacetabular osteotomy: prospective studies examining projected load-bearing area, bone density, cartilage thickness and migration. Acta Orthop Suppl 2008;79(329):4–43 - PubMed
-
- Wu JZ, Herzog W, Epstein M. Joint contact mechanics in the early stages of osteoarthritis. Med Eng Phys 2000;22(1):1–12 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
