

doi: 10.1186/1749-7922-5-11.
Acute gallbladder perforation with gallstones spillage in a cirrhotic patient
Affiliations
- PMID: 20416108
- PMCID: PMC2867990
- DOI: 10.1186/1749-7922-5-11
Item in Clipboard
Acute gallbladder perforation with gallstones spillage in a cirrhotic patient
World J Emerg Surg.
.
Abstract
Gallbladder perforation is a rare complication of cholecystitis and cholelithiasis. The high morbidity and mortality rates associated with this condition are due to delays in diagnosis and treatment since signs and symptoms of perforation do not differ significantly from those of uncomplicated cholecystitis. We report on a patient who was affected by Child-Pugh A alcoholic liver cirrhosis and who developed an acute gallbladder perforation with spillage of stones into the peritoneal cavity and give a review of the current literature.
Figures
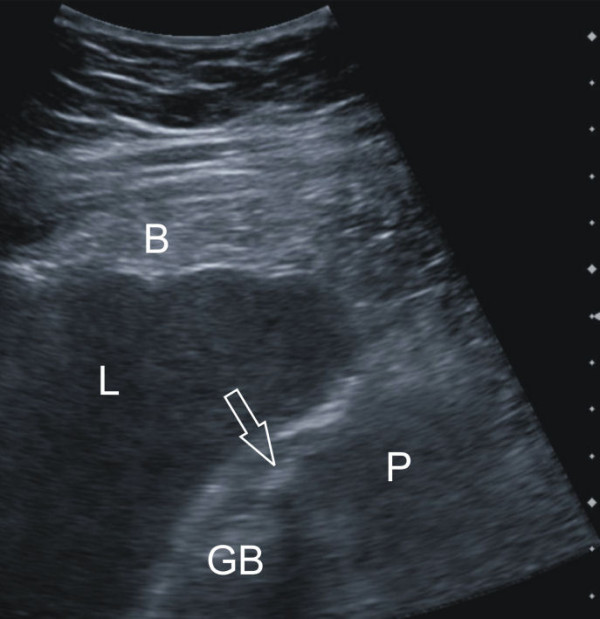
Sonography of the abdomen. This was performed after admission to our surgical department. Because of the lack of dorsal ultrasound reinforcement, the mass (P) surrounding the gallbladder (GB) was considered to be blood, pus or less likely tumorous soft tissue, not ascites. The transparent arrow indicates a stone.
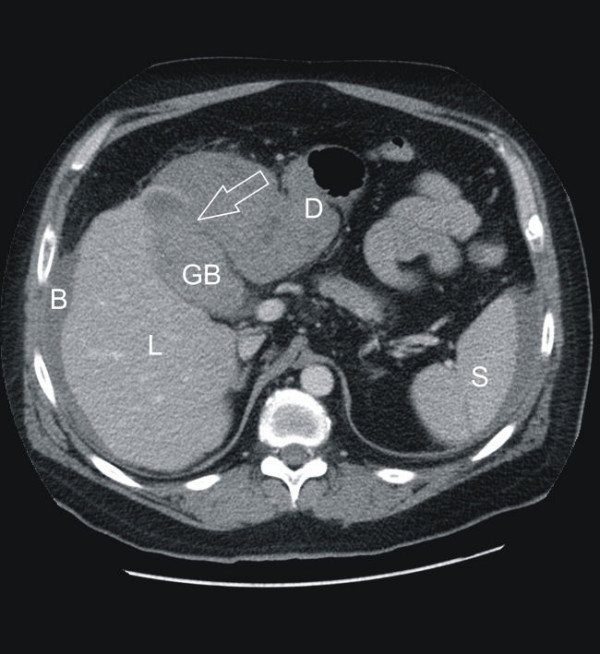
Computed tomography (CT) of the abdomen (a: axial slice). L = liver, GB = gallbladder, D = duodenum, S = spleen, B = blood. The perforation site is indicated by the transparent arrow.
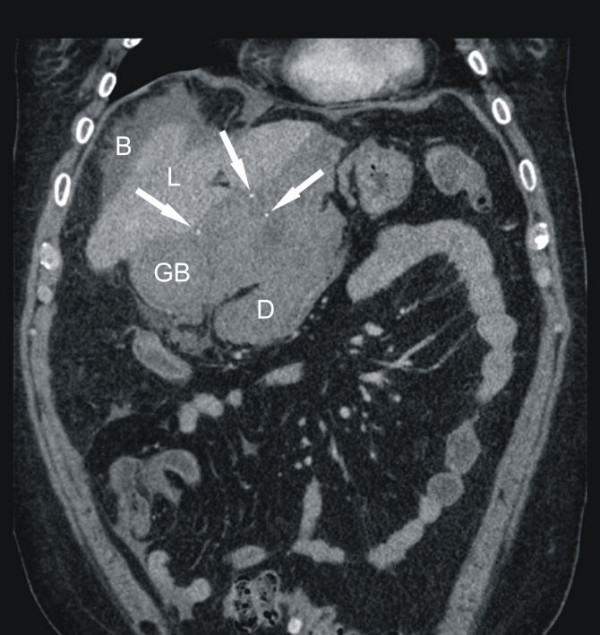
Computed tomography (CT) of the abdomen (coronal reformation). L = liver, GB = gallbladder, D = duodenum, S = spleen, B = blood. Several calcified stones are appreciated outside the gallbladder (solid arrows in figure 2b). Notice also progredient hyperdense fluids surrounding liver and spleen (B), altogether making the diagnosis of free gallbladder perforation obvious.

Intraoperative picture of the fluid from the patient's abdomen containing stones and clotted blood.
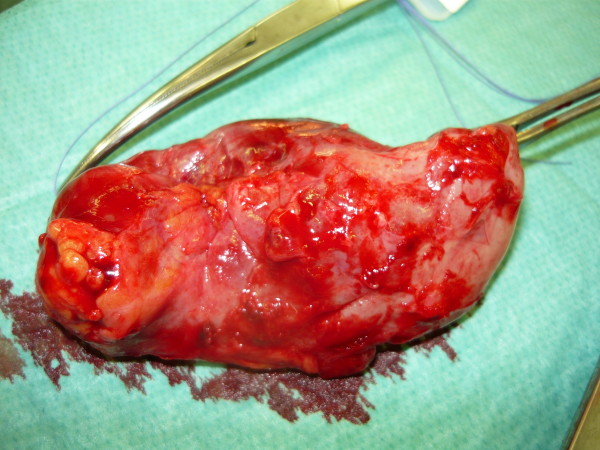
Intraoperative picture: the perforated gallbladder.
References
-
- Bakalakos EA, Melvin WS, Kirkpatrick R. Liver abscess secondary to intrahepatic perforation of the gallbladder, presenting as a liver mass. Am J Gastroenterol. 1996;91:1644–1646. - PubMed
-
- Gore RM, Ghahremani GG, Joseph AE, Nemcek AA Jr, Marn CS, Vogelzang RL. Acquired malposition of the colon and gallbladder in patients with cirrhosis: CT findings and clinical implications. Radiology. 1989;171:739–742. - PubMed
LinkOut - more resources
Full Text Sources
