

Isoflurane anesthesia does not satisfy the homeostatic need for rapid eye movement sleep
- PMID: 20418293
- PMCID: PMC3767968
- DOI: 10.1213/ANE.0b013e3181d3e861
Isoflurane anesthesia does not satisfy the homeostatic need for rapid eye movement sleep
Abstract
Background: Sleep and general anesthesia are distinct states of consciousness that share many traits. Prior studies suggest that propofol anesthesia facilitates recovery from rapid eye movement (REM) and non-REM (NREM) sleep deprivation, but the effects of inhaled anesthetics have not yet been studied. We tested the hypothesis that isoflurane anesthesia would also facilitate recovery from REM sleep deprivation.
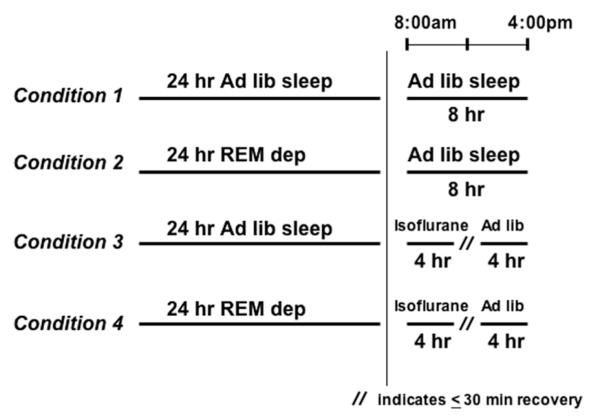
Methods: Six rats were implanted with superficial cortical, deep hippocampal, and nuchal muscle electrodes. Animals were deprived of REM sleep for 24 hours and then (1) allowed to sleep ad libitum for 8 hours or (2) were immediately anesthetized with isoflurane for a 4-hour period followed by ad libitum sleep for 4 hours. The percentage of REM and NREM sleep after the protocols was compared with similar conditions without sleep deprivation. Hippocampal activity during isoflurane anesthesia was also compared with activity during REM sleep and active waking.
Results: Recovery after deprivation was associated with a 5.7-fold increase (P = 0.0005) in REM sleep in the first 2 hours and a 2.6-fold increase (P = 0.004) in the following 2 hours. Animals that underwent isoflurane anesthesia after deprivation demonstrated a 3.6-fold increase (P = 0.001) in REM sleep in the first 2 hours of recovery and a 2.2-fold increase (P = 0.003) in the second 2 hours. There were no significant differences in REM sleep rebound between the first 4 hours after deprivation and the first 4 hours after both deprivation and isoflurane anesthesia. Hippocampal activity during isoflurane anesthesia was not affected by REM sleep deprivation, and the probability distribution of events during anesthesia was more similar to that of waking than to REM sleep.
Conclusion: Unlike propofol, isoflurane does not satisfy the homeostatic need for REM sleep. Furthermore, the regulation and organization of hippocampal events during anesthesia are unlike sleep. We conclude that different anesthetics have distinct interfaces with sleep.
Figures



References
-
- Lydic R, Baghdoyan HA. Sleep, anesthesiology, and the neurobiology of arousal state control. Anesthesiology. 2005;103:1268–95. - PubMed
-
- Franks NP. General anaesthesia: from molecular targets to neuronal pathways of sleep and arousal. Nat Rev Neurosci. 2008;9:370–86. - PubMed
-
- Rechtschaffen A, Bergmann BM, Gilliland MA, Bauer K. Effects of method, duration, and sleep stage on rebounds from sleep deprivation in the rat. Sleep. 1999;22:11–31. - PubMed
-
- Koblin DD. Urethane: help or hindrance? Anesth Analg. 2002;94:241–2. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
