

Fetal cardiac arrhythmia detection and in utero therapy
- PMID: 20418904
- PMCID: PMC2995324
- DOI: 10.1038/nrcardio.2010.32
Fetal cardiac arrhythmia detection and in utero therapy
Abstract
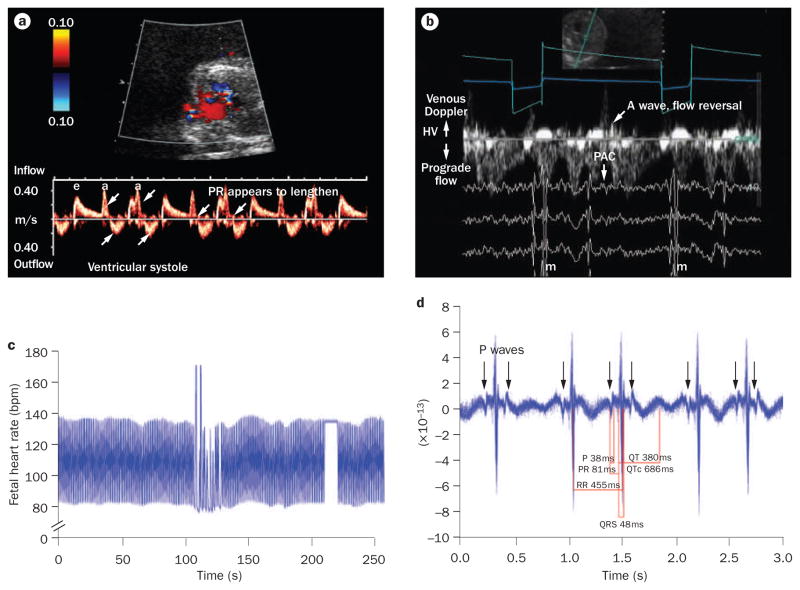
The human fetal heart develops arrhythmias and conduction disturbances in response to ischemia, inflammation, electrolyte disturbances, altered load states, structural defects, inherited genetic conditions, and many other causes. Yet sinus rhythm is present without altered rate or rhythm in some of the most serious electrophysiological diseases, which makes detection of diseases of the fetal conduction system challenging in the absence of magnetocardiographic or electrocardiographic recording techniques. Life-threatening changes in QRS or QT intervals can be completely unrecognized if heart rate is the only feature to be altered. For many fetal arrhythmias, echocardiography alone can assess important clinical parameters for diagnosis. Appropriate treatment of the fetus requires awareness of arrhythmia characteristics, mechanisms, and potential associations. Criteria to define fetal bradycardia specific to gestational age are now available and may allow detection of ion channelopathies, which are associated with fetal and neonatal bradycardia. Ectopic beats, once thought to be entirely benign, are now recognized to have important pathologic associations. Fetal tachyarrhythmias can now be defined precisely for mechanism-specific therapy and for subsequent monitoring of response. This article reviews the current and future diagnostic techniques and pharmacologic treatments for fetal arrhythmia.
Conflict of interest statement
The authors and the Journal Editor B. Mearns declare no competing interests. The CME questions author D. Lie has served as a nonproduct speaker for “Topics in Health” for Merck Speaker Services.
Figures
References
-
- Cuneo BF, et al. Prenatal diagnosis and in utero treatment of torsades de pointes associated with congenital long QT syndrome. Am J Cardiol. 2003;91:1395–1398. - PubMed
-
- Hamada H, et al. Prenatal diagnosis of long QT syndrome using fetal magnetocardiography. Prenat Diagn. 1999;19:677–680. - PubMed
-
- Horigome H, Iwashita H, Yoshinaga M, Shimizu W. Magnetocardiographic demonstration of torsade de pointes in a fetus with congenital long QT syndrome. J Cardiovasc Electrophysiol. 2008;19:334–335. - PubMed
-
- Hosono T, Shinto M, Chiba Y, Kandori A, Tsukada K. Prenatal diagnosis of fetal complete atrioventricular block with QT prolongation and alternating ventricular pacemakers using multi-channel magnetocardiography and current-arrow maps. Fetal Diagn Ther. 2002;17:173–176. - PubMed
-
- Miller TE, et al. Recurrent third-trimester fetal loss and maternal mosaicism for long-QT syndrome. Circulation. 2004;109:3029–3034. - PubMed
