

Temporal variability of human vaginal bacteria and relationship with bacterial vaginosis
- PMID: 20419168
- PMCID: PMC2855365
- DOI: 10.1371/journal.pone.0010197
Temporal variability of human vaginal bacteria and relationship with bacterial vaginosis
Abstract
Background: Little is known about short-term bacterial fluctuations in the human vagina. This study used PCR to assess the variability in concentrations of key vaginal bacteria in healthy women and the immediate response to antibiotic treatment in women with bacterial vaginosis (BV).
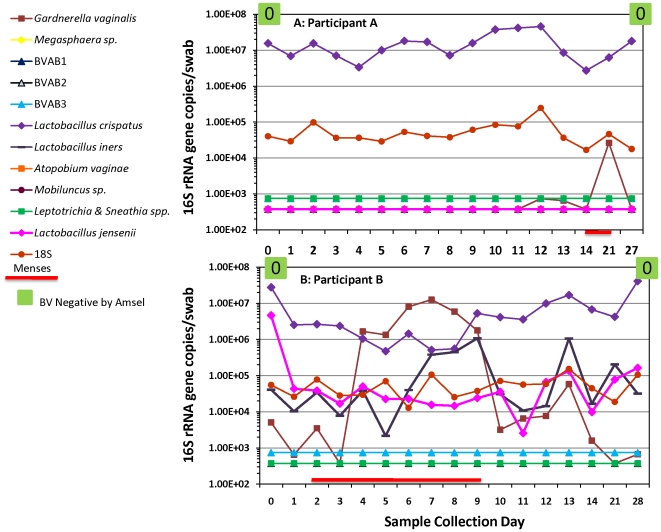
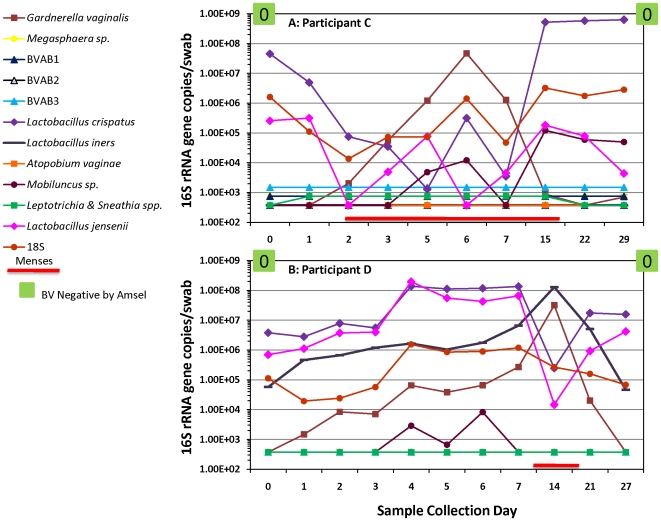
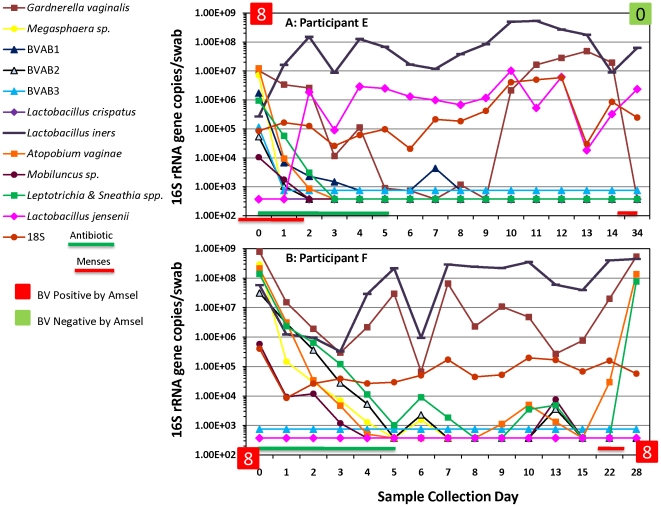
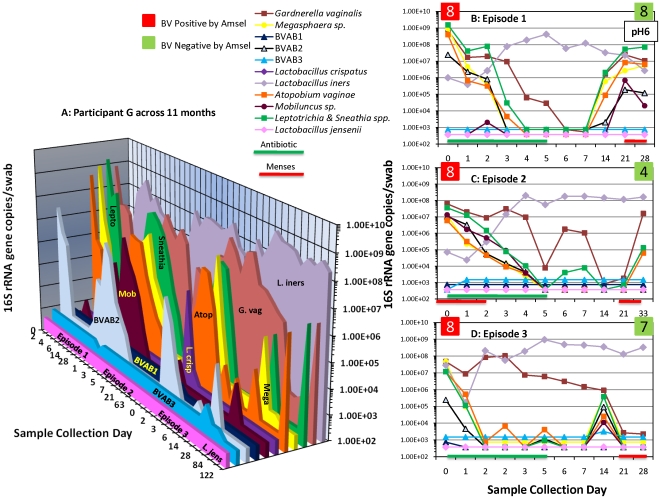
Methodology/principal findings: Twenty-two women assessed for BV using Amsel's criteria were evaluated daily for 7 or 14 days, then at 2, 3 and 4 weeks, using a panel of 11 bacterium-specific quantitative PCR assays. Participants with BV were treated with 5 days of intravaginal metronidazole. Participants without BV had vaginal biotas dominated by lactobacilli, whose levels fluctuated with menses. With onset of menstruation, quantities of Lactobacillus jensenii and Lactobacillus crispatus decreased and were found to be inversely related to Gardnerella vaginalis concentrations (p<0.001). Women with BV had a variety of fastidious bacteria whose concentrations dropped below detection thresholds 1-5 days after starting metronidazole. Recurrent BV was characterized by initial profound decreases of BV-associated bacteria after treatment followed by subsequent increases at relapse.
Conclusions/significance: The microbiota of the human vagina can be highly dynamic. Healthy women are colonized with Lactobacillus species, but levels can change dramatically over a month. Marked increases in G. vaginalis were observed during menses. Participants with BV have diverse communities of fastidious bacteria that are depleted by vaginal metronidazole therapy. Women with recurrent BV initially respond to antibiotic treatment with steep declines in bacterial concentrations, but these bacteria later reemerge, suggesting that antibiotic resistance in these bacteria is not an important factor mediating BV recurrence.
Conflict of interest statement
Figures
References
-
- Koumans EH, Sternberg M, Bruce C, McQuillan G, Kendrick J, et al. The prevalence of bacterial vaginosis in the United States, 2001–2004; associations with symptoms, sexual behaviors, and reproductive health. Sex Transm Dis. 2007;34:864–869. - PubMed
-
- Hillier SL, Nugent RP, Eschenbach DA, Krohn MA, Gibbs RS, et al. Association between bacterial vaginosis and preterm delivery of a low-birth-weight infant. The Vaginal Infections and Prematurity Study Group. N Engl J Med. 1995;333:1737–1742. - PubMed
-
- Taha TE, Hoover DR, Dallabetta GA, Kumwenda NI, Mtimavalye LA, et al. Bacterial vaginosis and disturbances of vaginal flora: association with increased acquisition of HIV. AIDS. 1998;12:1699–1706. - PubMed
-
- Haggerty CL, Hillier SL, Bass DC, Ness RB. Bacterial vaginosis and anaerobic bacteria are associated with endometritis. Clin Infec Dis. 2004;39:990–995. - PubMed
-
- Hillier S, Marrazzo JM, Holmes KK. Bacterial vaginosis. In: Holmes KK, Sparling P-A, editors. Sexually Transmitted Diseases. New York: McGraw-Hill; 2008. pp. 737–768.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
