

Direct peritoneal resuscitation accelerates primary abdominal wall closure after damage control surgery
- PMID: 20421025
- PMCID: PMC3471545
- DOI: 10.1016/j.jamcollsurg.2010.01.014
Direct peritoneal resuscitation accelerates primary abdominal wall closure after damage control surgery
Abstract
Background: Damage control surgery is a staged approach to the trauma patient in extremis that improves survival, but leads to open abdominal wounds that are difficult to manage. We evaluated whether directed peritoneal resuscitation (DPR) when used as a resuscitation strategy in severely injured trauma patients with hemorrhagic shock requiring damage control surgery would affect the amount of and timing of resuscitation and/or show benefits in time to abdominal closure and reduction of intra-abdominal complications.
Study design: A retrospective case-matched study of patients undergoing damage control surgery for hemorrhagic shock secondary to trauma between January 2005 and December 2008 was performed. Twenty patients undergoing standardized wound closure and adjunctive DPR were identified and matched to 40 controls by Injury Severity Score, age, gender, and mechanism of injury. A single early death was excluded because of inability to control ongoing hemorrhage.
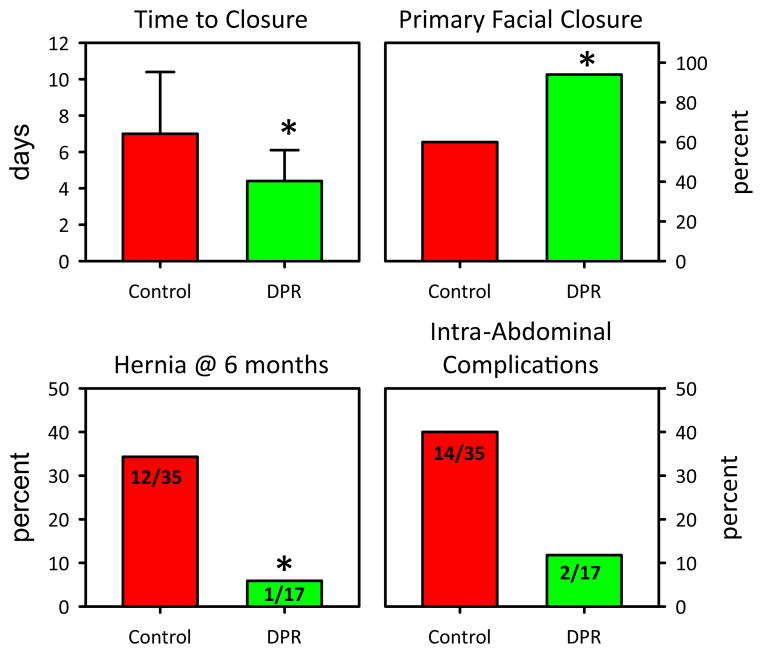
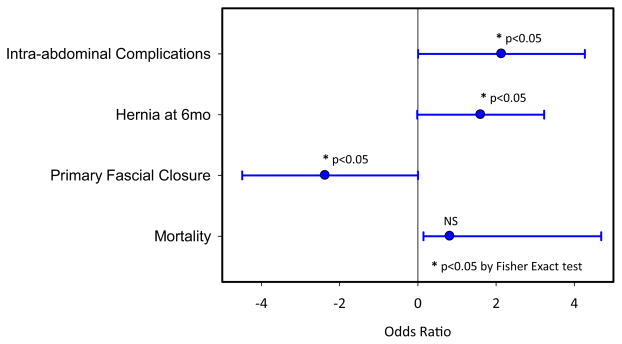
Results: There were no differences in age, gender, or mechanism of injury between the groups. Injury Severity Score (35.07 +/- 17.1 versus DPR 34.95 +/- 16.95; p = 0.82) and packed red blood cell administration in 24 hours (23.8 +/- 14.35 U versus DPR 26.9 +/- 14.1 U; p = 0.43) were similar between the groups. Presenting pH was similar between the study group and the DPR group (7.24 +/- 0.13 d versus DPR 7.26 +/- 0.11; p = 0.8). Time to definitive abdominal closure was significantly less in the DPR group compared with controls (DPR: 4.35 +/- 1.6 d versus 7.05 +/- 3.31; p < 0.003). DPR also allowed for a higher rate of primary fascial closure, lower intra-abdominal complication rate, and lower rate of ventral hernia formation at 6 months. Adjunctive DPR afforded a definitive wound closure advantage compared with Wittmann patch closure techniques (DPR 4.35 +/- 1.6 versus Wittmann patch 6.375 +/- 1.3; p = 0.004).
Conclusions: The addition of adjunctive DPR to the damage control strategy shortens the interval to definitive fascial closure without affecting overall resuscitation volumes. As a result, this mitigates intra-abdominal complications associated with open abdomen and damage control surgery and affords better patient outcomes.
Copyright 2010 American College of Surgeons. All rights reserved.
Figures
References
-
- Shires GT. Shock and metabolism. Surg Gynecol Obstet. 1967;124:284–287. - PubMed
-
- Brand ED, Shuh Tk, Avery MC. Reversal of postoligemic shock in the cat by hypervenobaric massive fluid therapy. Am J Physiol. 1966;211:1232–1240. - PubMed
-
- Wolfman EF, Neill SA, Heaps DK. Donor blood and isotonic salt solution. Effect on survival after hemorrhagic shock and operation. Arch Surg. 1963;86:869–873. - PubMed
-
- Foy H. Reinforced silicone elastomer sheeting, an improved method of temporary abdominal closure in damage control laparotomy. Am J Surg. 2003;185:498–501. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
