

Failure to perform cholecystectomy for acute cholecystitis in elderly patients is associated with increased morbidity, mortality, and cost
- PMID: 20421027
- PMCID: PMC2866125
- DOI: 10.1016/j.jamcollsurg.2009.12.031
Failure to perform cholecystectomy for acute cholecystitis in elderly patients is associated with increased morbidity, mortality, and cost
Abstract
Background: Cholecystectomy during initial hospitalization is the current recommended therapy for acute cholecystitis. The rate of cholecystectomy and subsequent health care trajectory in elderly patients with acute cholecystitis has not been evaluated.
Study design: We used 5% national Medicare sample claims data from 1996 to 2005 to identify a cohort of patients aged 66 years and older, requiring urgent or emergent admission for acute cholecystitis. We evaluated cholecystectomy rates on initial hospitalization, factors independently predicting receipt of cholecystectomy, factors predicting further gallstone-related complications, and 2-year survival in the cholecystectomy and no cholecystectomy groups in univariate and multivariate models.
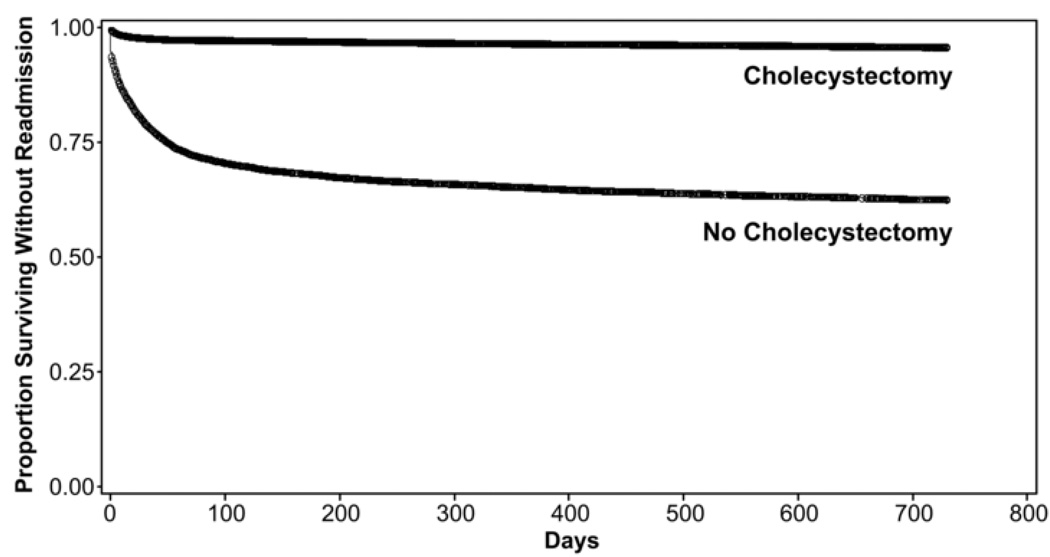
Results: There were 29,818 Medicare beneficiaries who were urgently or emergently admitted for acute cholecystitis from 1996 to 2005. Mean age was 77.7 +/- 7.3 years, 89% of patients were white, and 58% were female. Twenty-five percent of patients did not undergo cholecystectomy during the index admission. Lack of definitive therapy was associated with a 27% subsequent cholecystectomy rate and a 38% gallstone-related readmission rate in the 2 years after discharge; the readmission rate was only 4% in patients undergoing cholecystectomy (p < 0.0001). No cholecystectomy on initial hospitalization was associated with worse 2-year survival (hazard ratio 1.56, 95% CI 1.47 to 1.65) even after controlling for patient demographics and comorbidities. Readmissions led to an additional $7,000 in Medicare payments per readmission.
Conclusions: Our study demonstrated that 25% of cholecystectomies on Medicare beneficiaries were not performed on initial hospitalization, leading to readmissions in 38% of surviving patients. For patients requiring readmission, the percentage of open procedures was increased, and the additional Medicare payment was $7,000 per re-admission. Cholecystectomy for acute cholecystitis in elderly patients should be performed during initial hospitalization to prevent recurrent episodes of cholecystitis, multiple readmissions, higher readmission rates, and increased costs.
Copyright 2010 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures



References
-
- Steiner CA, Bass EB, Talamini MA, et al. Surgical rates and operative mortality for open and laparoscopic cholecystectomy in Maryland. N Engl J Med. 1994;330:403–408. - PubMed
-
- Gallstones and laparoscopic cholecystectomy. NIH Consensus Statement. 1992 - PubMed
-
- Chiang WK, Lee FM, Santen S. Cholelithiasis [EMedicine web site] 2008 [Accessed 07/28/09]; Available at: http://emedicine.medscape.com/article/774352-overview.
-
- Gracie WA, Ransohoff DF. The natural history of silent gallstones: the innocent gallstone is not a myth. N Engl J Med. 1982;307:798–800. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
