

Alternative strategies to reduce maternal mortality in India: a cost-effectiveness analysis
- PMID: 20421922
- PMCID: PMC2857650
- DOI: 10.1371/journal.pmed.1000264
Alternative strategies to reduce maternal mortality in India: a cost-effectiveness analysis
Abstract
Background: Approximately one-quarter of all pregnancy- and delivery-related maternal deaths worldwide occur in India. Taking into account the costs, feasibility, and operational complexity of alternative interventions, we estimate the clinical and population-level benefits associated with strategies to improve the safety of pregnancy and childbirth in India.
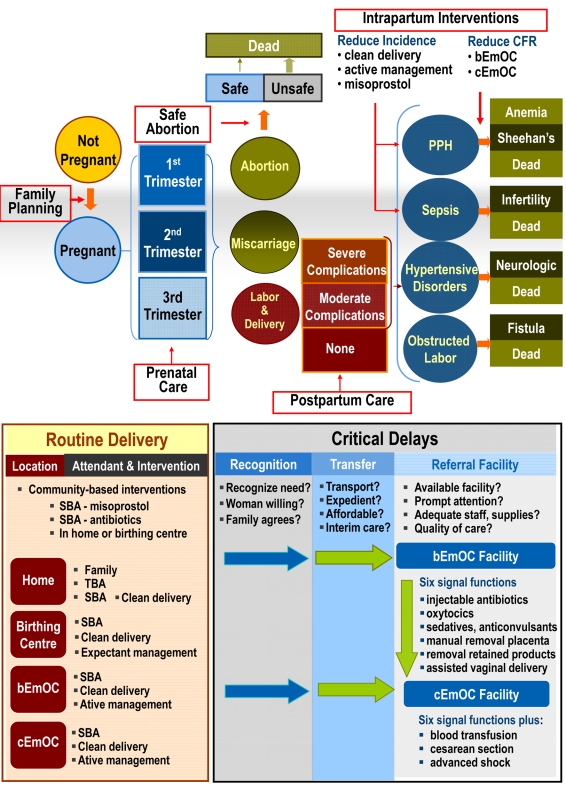
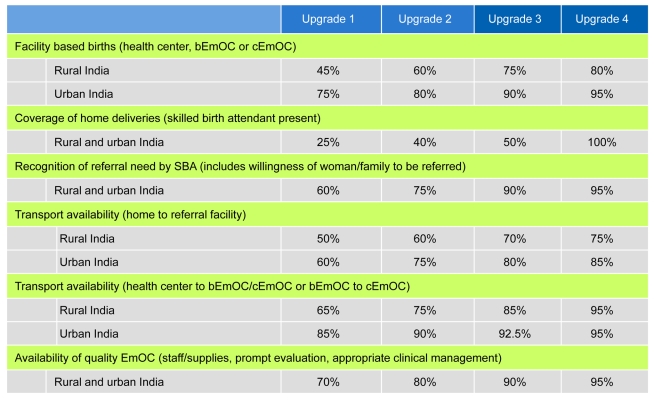
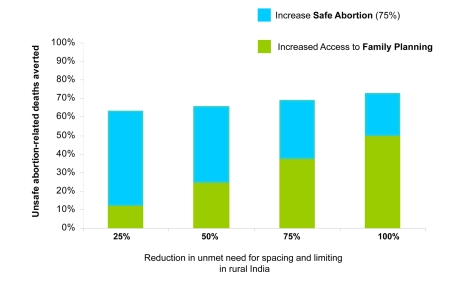
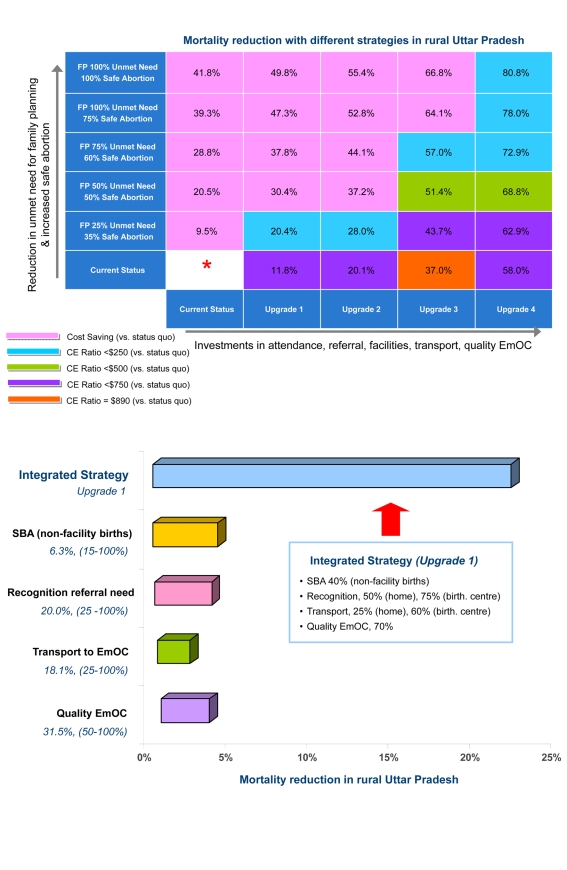
Methods and findings: Country- and region-specific data were synthesized using a computer-based model that simulates the natural history of pregnancy (both planned and unintended) and pregnancy- and childbirth-associated complications in individual women; and considers delivery location, attendant, and facility level. Model outcomes included clinical events, population measures, costs, and cost-effectiveness ratios. Separate models were adapted to urban and rural India using survey-based data (e.g., unmet need for birth spacing/limiting, facility births, skilled birth attendants). Model validation compared projected maternal indicators with empiric data. Strategies consisted of improving coverage of effective interventions that could be provided individually or packaged as integrated services, could reduce the incidence of a complication or its case fatality rate, and could include improved logistics such as reliable transport to an appropriate referral facility as well as recognition of referral need and quality of care. Increasing family planning was the most effective individual intervention to reduce pregnancy-related mortality. If over the next 5 y the unmet need for spacing and limiting births was met, more than 150,000 maternal deaths would be prevented; more than US$1 billion saved; and at least one of every two abortion-related deaths averted. Still, reductions in maternal mortality reached a threshold ( approximately 23%-35%) without including strategies that ensured reliable access to intrapartum and emergency obstetrical care (EmOC). An integrated and stepwise approach was identified that would ultimately prevent four of five maternal deaths; this approach coupled stepwise improvements in family planning and safe abortion with consecutively implemented strategies that incrementally increased skilled attendants, improved antenatal/postpartum care, shifted births away from home, and improved recognition of referral need, transport, and availability/quality of EmOC. The strategies in this approach ranged from being cost-saving to having incremental cost-effectiveness ratios less than US$500 per year of life saved (YLS), well below India's per capita gross domestic product (GDP), a common benchmark for cost-effectiveness.
Conclusions: Early intensive efforts to improve family planning and control of fertility choices and to provide safe abortion, accompanied by a paced systematic and stepwise effort to scale up capacity for integrated maternal health services over several years, is as cost-effective as childhood immunization or treatment of malaria, tuberculosis, or HIV. In just 5 y, more than 150,000 maternal deaths would be averted through increasing contraception rates to meet women's needs for spacing and limiting births; nearly US$1.5 billion would be saved by coupling safe abortion to aggressive family planning efforts; and with stepwise investments to improve access to pregnancy-related health services and to high-quality facility-based intrapartum care, more than 75% of maternal deaths could be prevented. If accomplished over the next decade, the lives of more than one million women would be saved.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization (WHO) 2007. Maternal mortality in 2005: estimates developed by WHO, UNICEF, UNFPA, and The World Bank. Available: http://www.who.int/whosis/mme_2005.pdf. Accessed 19 August 2009.
-
- Hill K, Thomas K, AbouZahr C, Walker N, Say L, et al. Estimates of maternal mortality worldwide between 1990 and 2005: an assessment of available data. Lancet. 2007;370:1311–1319. - PubMed
-
- United Nations (UN) Millennium Development Goals: Goal 5 (MDG 5). Improve maternal health. Available: http://www.un.org/millenniumgoals/maternal.shtml. Accessed 31 July 2009.
-
- World Health Organization (WHO) 2005. Millennium Development Goals and Health–India. Chapter III: Goal 5: improve maternal health. Geneva: WHO. Available: http://www.whoindia.org/LinkFiles/MDG_Chapter-03.pdf. Accessed 31 July 2009.
-
- Shiffman J, Ved R. The state of political priority for safe motherhood in India. BJOG. 2007;114:785–90. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
