

Partial volume correction strategies for quantitative FDG PET in oncology
- PMID: 20422184
- PMCID: PMC2918791
- DOI: 10.1007/s00259-010-1472-7
Partial volume correction strategies for quantitative FDG PET in oncology
Abstract
Purpose: Quantitative accuracy of positron emission tomography (PET) is affected by partial volume effects resulting in increased underestimation of the standardized uptake value (SUV) with decreasing tumour volume. The purpose of the present study was to assess accuracy and precision of different partial volume correction (PVC) methods.
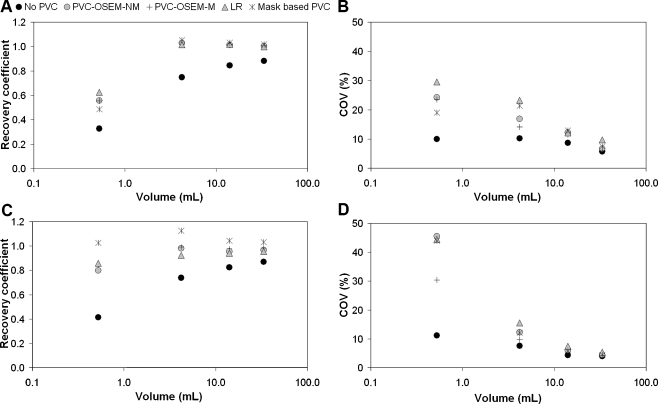
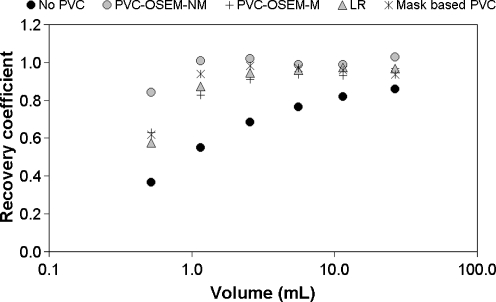
Methods: Three methods for PVC were evaluated: (1) inclusion of the point spread function (PSF) within the reconstruction, (2) iterative deconvolution of PET images and (3) calculation of spill-in and spill-out factors based on tumour masks. Simulations were based on a mathematical phantom with tumours of different sizes and shapes. Phantom experiments were performed in 2-D mode using the National Electrical Manufacturers Association (NEMA) NU2 image quality phantom containing six differently sized spheres. Clinical studies (2-D mode) included a test-retest study consisting of 10 patients with stage IIIB and IV non-small cell lung cancer and a response monitoring study consisting of 15 female breast cancer patients. In all studies tumour or sphere volumes of interest (VOI) were generated using VOI based on adaptive relative thresholds.
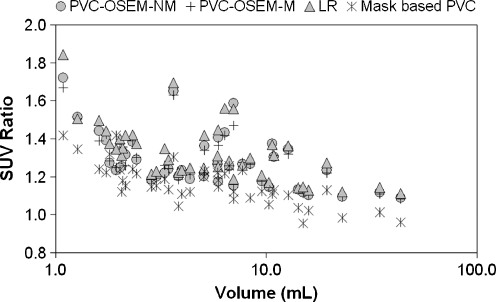
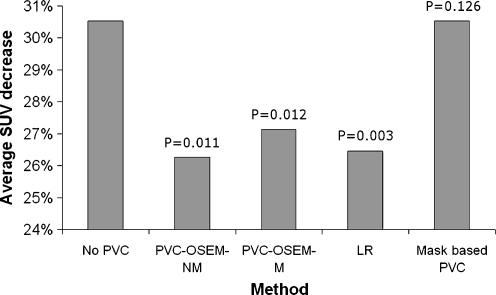
Results: Simulations and experiments provided similar results. All methods were able to accurately recover true SUV within 10% for spheres equal to and larger than 1 ml. Reconstruction-based recovery, however, provided up to twofold better precision than image-based methods. Clinical studies showed that PVC increased SUV by 5-80% depending on tumour size. Test-retest variability slightly worsened from 9.8 +/- 6.5 without to 10.8 +/- 7.9% with PVC. Finally, PVC resulted in slightly smaller SUV responses, i.e. from -30.5% without to -26.3% with PVC after the first cycle of treatment (p < 0.01).
Conclusion: PVC improves accuracy of SUV without decreasing (clinical) test-retest variability significantly and it has a small, but significant effect on observed tumour responses. Reconstruction-based PVC outperforms image-based methods, but requires dedicated reconstruction software. Image-based methods are good alternatives because of their ease of implementation and their similar performance in clinical studies.
Figures


References
-
- Hoekstra CJ, Paglianiti I, Hoekstra OS, Smit EF, Postmus PE, Teule GJ, et al. Monitoring response to therapy in cancer using [18F]-2-fluoro-2-deoxy-D-glucose and positron emission tomography: an overview of different analytical methods. Eur J Nucl Med. 2000;27(6):731–743. doi: 10.1007/s002590050570. - DOI - PubMed
-
- Lowe VJ, DeLong DM, Hoffman JM, Coleman RE. Optimum scanning protocol for FDG-PET evaluation of pulmonary malignancy. J Nucl Med. 1995;36(5):883–887. - PubMed
-
- Boellaard R, Krak NC, Hoekstra OS, Lammertsma AA. Effects of noise, image resolution, and ROI definition on the accuracy of standard uptake values: a simulation study. J Nucl Med. 2004;45(9):1519–1527. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
