

Pretargeted radioimmunotherapy for hematologic and other malignancies
- PMID: 20423225
- PMCID: PMC2936263
- DOI: 10.1089/cbr.2010.0759
Pretargeted radioimmunotherapy for hematologic and other malignancies
Abstract
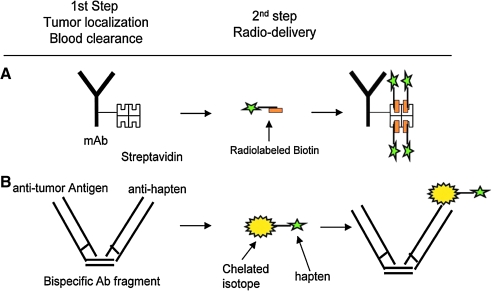
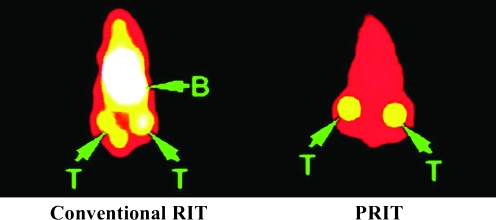
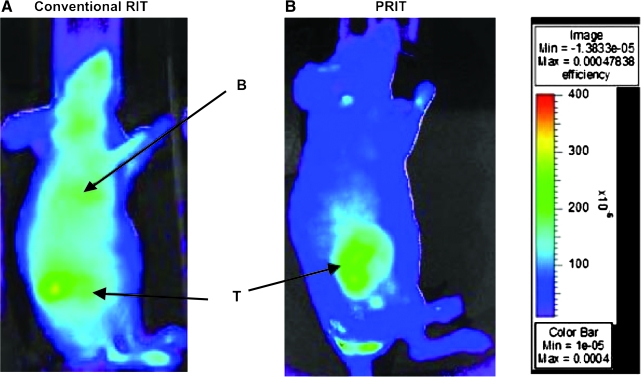
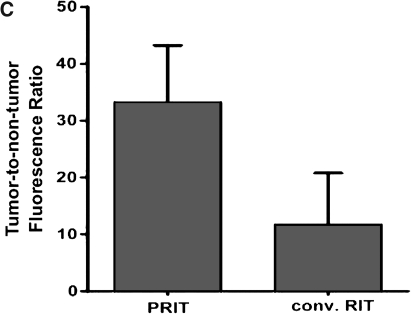
Radioimmunotherapy (RIT) has emerged as one of the most promising treatment options, particularly for hematologic malignancies. However, this approach has generally been limited by a suboptimal therapeutic index (target-to-nontarget ratio) and an inability to deliver sufficient radiation doses to tumors selectively. Pretargeted RIT (PRIT) circumvents these limitations by separating the targeting vehicle from the subsequently administered therapeutic radioisotope, which binds to the tumor-localized antibody or is quickly excreted if unbound. A growing number of preclinical proof-of-principle studies demonstrate that PRIT is feasible and safe and provides improved directed radionuclide delivery to malignant cells compared with conventional RIT while sparing normal cells from nonspecific radiotoxicity. Early phase clinical studies corroborate these preclinical findings and suggest better efficacy and lesser toxicities in patients with hematologic and other malignancies. With continued research, PRIT-based treatment strategies promise to become cornerstones to improved outcomes for cancer patients despite their complexities.
Figures


References
-
- Park SI. Press OW. Radioimmunotherapy for treatment of B-cell lymphomas and other hematologic malignancies. Curr Opin Hematol. 2007;14:632. - PubMed
-
- Green DJ. Pagel JM. Pantelias A, et al. Pretargeted radioimmunotherapy for B-cell lymphomas. Clin Cancer Res. 2007;13:5598s. - PubMed
-
- Strand SE. Zanzonico P. Johnson TK. Pharmacokinetic modeling. Med Phys. 1993;20:515. - PubMed
-
- Chinol M. Grana C. Gennari R, et al. Pretargeted radio of cancer. In: Abrams PG, editor; Fritzberg AR, editor. Radioimmunotherapy of Cancer. New York: Marcel Dekker; 2000. p. 169.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
