

Growth hormone treatment does not affect incidences of middle ear disease or hearing loss in infants and toddlers with Turner syndrome
- PMID: 20424424
- PMCID: PMC2914351
- DOI: 10.1159/000313964
Growth hormone treatment does not affect incidences of middle ear disease or hearing loss in infants and toddlers with Turner syndrome
Abstract
Context: No randomized, controlled, prospective study has evaluated the effect of growth hormone (GH) on the rates of middle ear (ME) disease and hearing loss in girls with Turner syndrome (TS).
Design: A 2-year, prospective, randomized, controlled, open-label, multicenter, clinical trial ('Toddler Turner Study'; August 1999 to August 2003) was carried out.
Setting: The study was conducted at 11 US pediatric endocrine centers.
Subjects: Eighty-eight girls with TS, aged 9 months to 4 years, were enrolled.
Intervention: The interventions comprised recombinant GH (50 microg/kg/day, n = 45) or no treatment (n = 43) for 2 years.
Main outcome measures: The outcome measures included occurrence rates of ear-related problems, otitis media (OM) and associated antibiotic treatments, tympanometric assessment of ME function and hearing assessment by audiology.
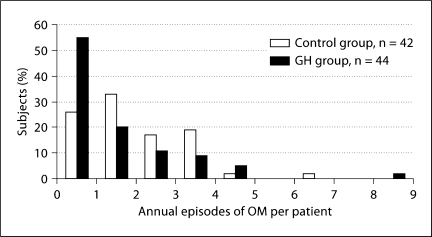
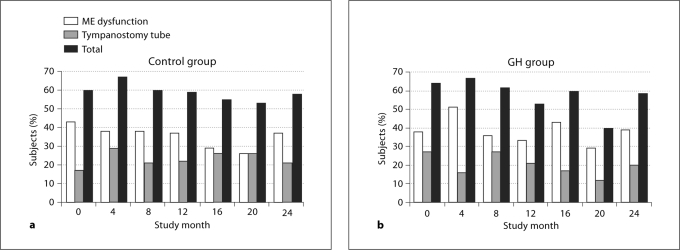
Results: At baseline, 57% of the girls (mean age = 1.98 +/- 1.00 years) had a history of recurrent OM, 33% had undergone tympanostomy tube (t-tube) insertion and 27% had abnormal hearing. There was no significant difference between the treatment groups for annual incidence of OM episodes (untreated control: 1.9 +/- 1.4; GH-treated: 1.5 +/- 1.6, p = 0.17). A quarter of the subjects underwent ear surgeries (mainly t-tube insertions) during the study. Recurrent or persistent abnormality of ME function on tympanometry was present in 28-45% of the girls without t-tubes at the 6 postbaseline visits. Hearing deficits were found in 19-32% of the girls at the annual postbaseline visits. Most of these were conductive deficits, however, 2 girls had findings consistent with sensorineural hearing loss, which was evident before 3 years of age.
Conclusions: Ear and hearing problems are common in infants and toddlers with TS and are not significantly influenced by GH treatment. Girls with TS need early, regular and thorough ME monitoring by their primary care provider and/or otolaryngologist, and at least annual hearing evaluations by a pediatric audiologist.
Copyright 2010 S. Karger AG, Basel.
Figures
References
-
- Nielsen J, Wohlert M. Chromosome abnormalities found among 34,910 newborn children: results from a 13-year incidence study in Aarhus, Denmark. Hum Genet. 1991;87:81–83. - PubMed
-
- Davenport ML, Calikoglu AS. Turner Syndrome. In: Pescovitz OH, Eugster EA, editors. Pediatric Endocrinology. Mechanisms, Manifestations, and Management. Philadelphia: Lippincott Williams & Wilkins; 2004. pp. 203–223.
-
- Bondy CA. Care of girls and women with Turner syndrome: a guideline of the Turner syndrome study group. J Clin Endocrinol Metab. 2007;92:10–25. - PubMed
-
- Carel JC, Ecosse E, Bastie-Sigeac I, Cabrol S, Tauber M, Léger J, Nicolino M, Brauner R, Chaussain JL, Coste J. Quality of life determinants in young women with Turner's syndrome after growth hormone treatment: results of the StaTur population-based cohort study. J Clin Endocrinol Metab. 2005;90:1992–1997. - PubMed
-
- Güngör N, Böke B, Belgin E, Tunçbilek E. High frequency hearing loss in Ullrich-Turner syndrome. Eur J Pediatr. 2000;159:740–744. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
