

Surgery for colorectal liver metastases
- PMID: 20424612
- PMCID: PMC2865767
- DOI: 10.1038/sj.bjc.6605659
Surgery for colorectal liver metastases
Abstract
In this review the surgery of colorectal liver metastases is discussed. It has long been known that liver surgery can cure metastatic colorectal cancer although in only a small proportion of the population with the disease. However with better understanding of the natural history of the condition and advances in technique more patients can have safe, potentially curative surgery. The multidiscipline management of patients with effective chemotherapy has led to more patients benefiting from surgery after reducing the size of the metastases and allowing operation on patients who were previously inoperable. Chemotherapy also improves at least the medium-term outcome in those who are operable at the outset. Minimally invasive techniques have been developed so that major hepatectomy may be accomplished in up to half of such cases with a very short hospital stay and limited interference with quality of life. Lastly, using portal vein embolisation to cause hypertrophy of the future liver remnant and on occasions combining it with staged liver resection allows potentially curative surgery on patients who previously could not have survived resection. These developments have led to more patients being cured of advanced colorectal cancer.
Figures
References
-
- Abu Hilal M, Pearce NW (2008) Laparoscopic left lateral liver sectionectomy: a safe, efficient, reproducible technique. Dig Surg 25: 305–308 - PubMed
-
- Abu Hilal M, Underwood T, Zuccaro M, Primrose J, Pearce N (2010) Short- and medium-term results of totally laparoscopic resection for colorectal liver metastases. Br J Surg, doi:10.1002/bjs.7034 - PubMed
-
- Adam R, Wicherts DA, de Haas RJ, Ciacio O, Levi F, Paule B, Ducreux M, Azoulay D, Bismuth H, Castaing D (2009) Patients with initially unresectable colorectal liver metastases: is there a possibility of cure? J Clin Oncol 27: 1829–1835 - PubMed
-
- Benoist S, Brouquet A, Penna C, Julie C, El Hajjam M, Chagnon S, Mitry E, Rougier P, Nordlinger B (2006) Complete response of colorectal liver metastases after chemotherapy: does it mean cure? J Clin Oncol 24: 3939–3945 - PubMed
-
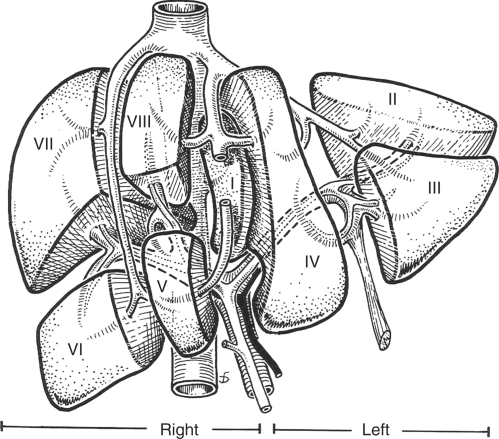
- Couinaud C, Delmas A, Patel J (1957) Le foie: Études anatomiques et chirurgicales. Masson: Paris
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
