

Presence of an in situ component is associated with reduced biological aggressiveness of size-matched invasive breast cancer
- PMID: 20424617
- PMCID: PMC2865763
- DOI: 10.1038/sj.bjc.6605655
Presence of an in situ component is associated with reduced biological aggressiveness of size-matched invasive breast cancer
Abstract
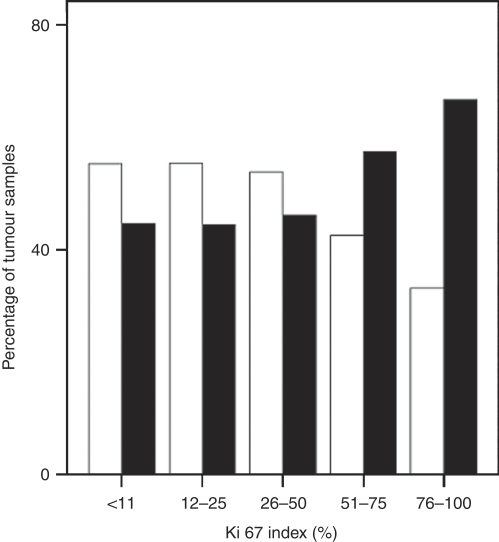
Background: The metastatic propensity of invasive ductal carcinoma (IDC) of the breast correlates with axillary node involvement and with expression of the proliferation antigen Ki-67, whereas ductal carcinoma in situ (DCIS) is non-metastasising. To clarify whether concomitant DCIS affects IDC prognosis, we compared Ki-67 expression and node status of size-matched IDC subgroups either with DCIS (IDC-DCIS) or without DCIS (pure IDC).
Methods: We analysed data from 1355 breast cancer patients. End points were defined by the association of IDC (with or without DCIS) with grade, nodal status, Ki-67, and ER/HER2.
Results: Size-matched IDC-DCIS was more likely than pure IDC to be screen detected (P=0.03), to occur in pre-menopausal women (P=0.002), and to be either ER-positive (P=0.002) or HER2-positive (P<0.0005), but less likely to be treated with breast-conserving surgery (P=0.004). Grade and Ki-67 were lower in IDC-DCIS than in pure IDC (P=0.02), and declined as the DCIS enlarged (P<0.01). Node involvement and lymphovascular invasion in IDC-DCIS increased with the size ratio of IDC to DCIS (P<0.01). A 60-month cancer-specific survival favoured IDC-DCIS over size-matched pure IDC (97.4 vs 96.0%).
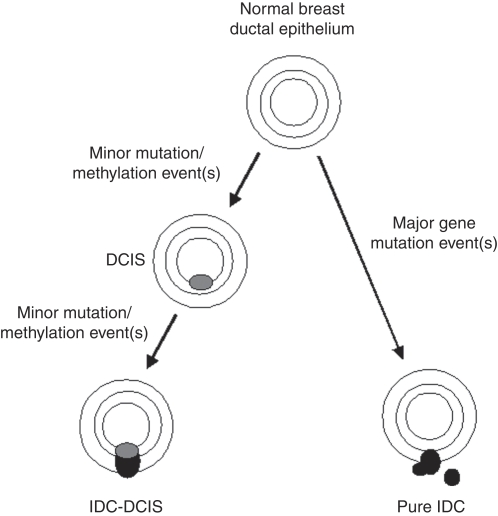
Conclusion: IDC co-existing with DCIS is characterised by lower proliferation and metastatic potential than size-matched pure IDC, especially if the ratio of DCIS to IDC size is high. We submit that IDC-DCIS is biologically distinct from pure IDC, and propose an incremental molecular pathogenesis of IDC-DCIS evolution involving an intermediate DCIS precursor that remains dependent for replication on upstream mitogens.
Conflict of interest statement
The authors declare no conflict of interest
Figures
References
-
- Alexe G, Dalgin GS, Ganesan S, Delisi C, Bhanot G (2007) Analysis of breast cancer progression using principal component analysis and clustering. J Biosci 32: 1027–1039 - PubMed
-
- Allred DC, Mohsin SK, Fuqua SA (2001) Histological and biological evolution of human premalignant breast disease. Endocr Relat Cancer 8: 47–61 - PubMed
-
- Aubele M, Mattis A, Zitzelsberger H, Walch A, Kremer M, Welzl G, Hofler H, Werner M (2000) Extensive ductal carcinoma in situ with small foci of invasive ductal carcinoma: evidence of genetic resemblance by CGH. Int J Cancer 85: 82–86 - PubMed
-
- Barnard NJ, Hall PA, Lemoine NR, Kadar N (1987) Proliferative index in breast carcinoma determined in situ by Ki67 immunostaining and its relationship to clinical and pathological variables. J Pathol 152: 287–295 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
