

Imaging lung disease in systemic sclerosis
- PMID: 20425026
- PMCID: PMC2845885
- DOI: 10.1007/s11926-010-0095-0
Imaging lung disease in systemic sclerosis
Abstract
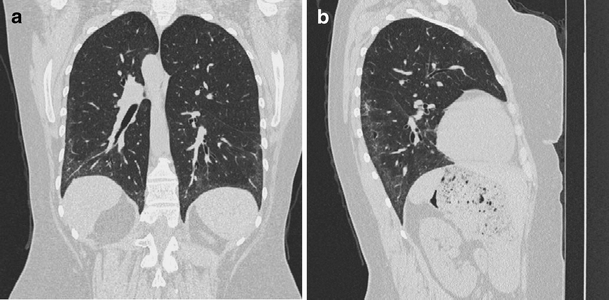
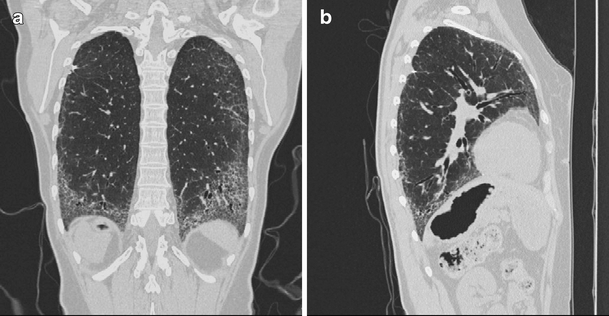
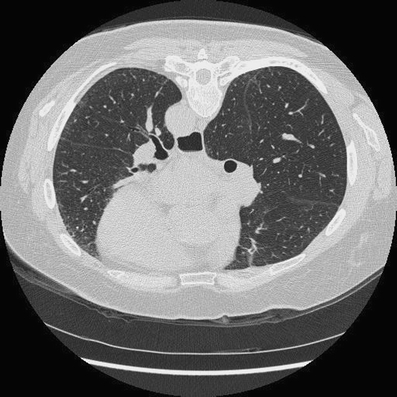
Interstitial lung disease and pulmonary hypertension (PH) are the most common cardiopulmonary findings in patients with systemic sclerosis (SSc). About two thirds of patients suffering from SSc develop scleroderma interstitial lung disease. PH is present in about 20% of SSc patients and is typically associated with severe lung disease, although it may be an isolated manifestation of SSc. High-resolution CT scanning is a key method for evaluating chest involvement. There are four roles of imaging in scleroderma interstitial lung disease: 1) detection of lung involvement, 2) identification of patients likely to respond to treatment, 3) assessment of treatment efficacy, and 4) exclusion of other significant diseases to include PH and cardiac and esophageal abnormalities.
Figures
References
-
- Silver RM, Miller KS. Lung involvement in systemic sclerosis. Rheum Dis Clin North Am. 1990;16:199–216. - PubMed
-
- Gilliland BC, et al. Systemic sclerosis (scleroderma) In: Braunwald E, Fauci AS, Kasper DL, et al., editors. Harrison’s Principles of Internal Medicine. 15. New York: McGraw-Hill; 2001.
