

Management of low-grade glioma
- PMID: 20425038
- PMCID: PMC2857752
- DOI: 10.1007/s11910-010-0105-7
Management of low-grade glioma
Abstract
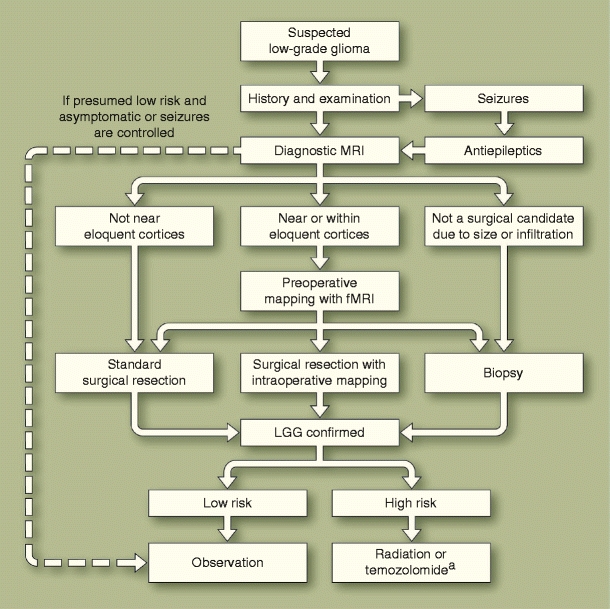
The optimal management of patients with low-grade glioma (LGG) is controversial. The controversy largely stems from the lack of well-designed clinical trials with adequate follow-up to account for the relatively long progression-free survival and overall survival of patients with LGG. Nonetheless, the literature increasingly suggests that expectant management is no longer optimal. Rather, there is mounting evidence supporting active management including consideration of surgical resection, radiotherapy, chemotherapy, molecular and histopathologic characterization, and use of modern imaging techniques for monitoring and prognostication. In particular, there is growing evidence favoring extensive surgical resection and increasing interest in the role of chemotherapy (especially temozolomide) in the management of these tumors. In this review, we critically analyze emerging trends in the literature with respect to management of LGG, with particular emphasis on reports published during the past year.
Figures
References
-
- Central Brain Tumor Registry of the United States: Statistical Report: Primary Brain Tumors in the United States, 2000–2004. Available at http://www.cbtrus.org/reports//2007-2008/2007report.pdf. Accessed February 2010.
-
- Shaw E, Arusell R, Scheithauer B, et al. Prospective randomized trial of low- versus high-dose radiation therapy in adults with supratentorial low-grade glioma: initial report of a North Central Cancer Treatment Group/Radiation Therapy Oncology Group/Eastern Cooperative Oncology Group study. J Clin Oncol. 2002;20:2267–2276. doi: 10.1200/JCO.2002.09.126. - DOI - PubMed
-
- Bauman G, Lote K, Larson D, et al. Pretreatment factors predict overall survival for patients with low-grade glioma: a recursive partitioning analysis. Int J Radiat Oncol Biol Phys. 1999;45:923–929. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
