

Electrical muscle stimulation prevents critical illness polyneuromyopathy: a randomized parallel intervention trial
- PMID: 20426834
- PMCID: PMC2887197
- DOI: 10.1186/cc8987
Electrical muscle stimulation prevents critical illness polyneuromyopathy: a randomized parallel intervention trial
Abstract
Introduction: Critical illness polyneuromyopathy (CIPNM) is a common complication of critical illness presenting with muscle weakness and is associated with increased duration of mechanical ventilation and weaning period. No preventive tool and no specific treatment have been proposed so far for CIPNM. Electrical muscle stimulation (EMS) has been shown to be beneficial in patients with severe chronic heart failure and chronic obstructive pulmonary disease. Aim of our study was to assess the efficacy of EMS in preventing CIPNM in critically ill patients.
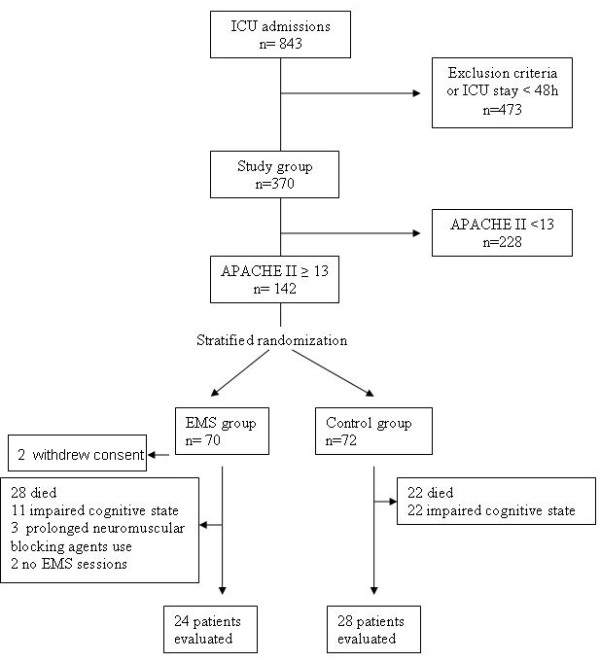
Methods: One hundred and forty consecutive critically ill patients with an APACHE II score >or= 13 were randomly assigned after stratification to the EMS group (n = 68) (age:61 +/- 19 years) (APACHE II:18 +/- 4, SOFA:9 +/- 3) or to the control group (n = 72) (age:58 +/- 18 years) (APACHE II:18 +/- 5, SOFA:9 +/- 3). Patients of the EMS group received daily EMS sessions. CIPNM was diagnosed clinically with the medical research council (MRC) scale for muscle strength (maximum score 60, <48/60 cut off for diagnosis) by two unblinded independent investigators. Duration of weaning from mechanical ventilation and intensive care unit (ICU) stay were recorded.
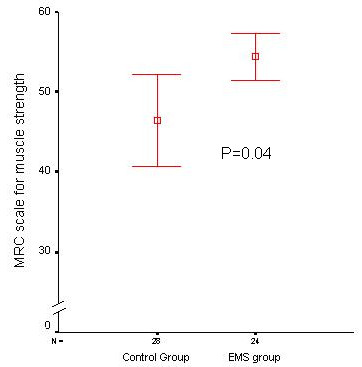
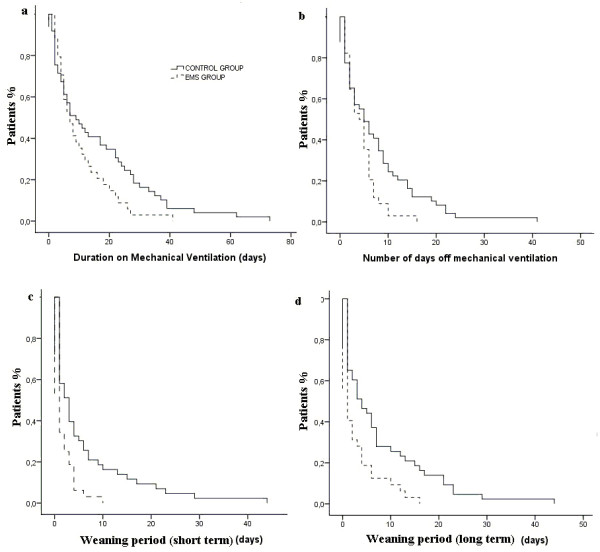
Results: Fifty two patients could be finally evaluated with MRC; 24 in the EMS group and 28 in the control group. CIPNM was diagnosed in 3 patients in the EMS group as compared to 11 patients in the control group (OR = 0.22; CI: 0.05 to 0.92, P = 0.04). The MRC score was significantly higher in patients of the EMS group as compared to the control group [58 (33 to 60) vs. 52 (2 to 60) respectively, median (range), P = 0.04). The weaning period was statistically significantly shorter in patients of the EMS group vs. the control group [1 (0 to 10) days vs. 3 (0 to 44) days, respectively, median (range), P = 0.003].
Conclusions: This study suggests that daily EMS sessions prevent the development of CIPNM in critically ill patients and also result in shorter duration of weaning. Further studies should evaluate which patients benefit more from EMS and explore the EMS characteristics most appropriate for preventing CIPNM.
Trial registration number: ClinicalTrials.gov NCT00882830.
Figures

Comment in
-
Have we found the prevention for intensive care unit-acquired paresis?Crit Care. 2010;14(3):160. doi: 10.1186/cc9005. Epub 2010 May 24. Crit Care. 2010. PMID: 20519035 Free PMC article.
-
Electrical muscle stimulation for prevention of critical illness polyneuropathy.Crit Care. 2010;14(4):428; author reply 428. doi: 10.1186/cc9081. Epub 2010 Jul 12. Crit Care. 2010. PMID: 20624326 Free PMC article. No abstract available.
References
-
- Ali NA, O'Brien JM Jr, Hoffmann SP, Phillips G, Garland A, Finley JC, Almoosa K, Hejal R, Wolf KM, Lemeshow S, Connors AF Jr, Marsh CB. Acquired weakness, handgrip strength, and mortality in critically ill patients. Am J Respir Crit Care Med. 2008;178:261–268. doi: 10.1164/rccm.200712-1829OC. - DOI - PubMed
-
- De Jonghe B, Sharshar T, Lefaucheur JP, Authier FJ, Durand-Zaleski I, Boussarsar M, Cerf C, Renaud E, Mesrati F, Carlet J, Raphaël JC, Outin H, Bastuji-Garin S. Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002;288:2859–2867. doi: 10.1001/jama.288.22.2859. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
