

A recruitment maneuver increases oxygenation after intubation of hypoxemic intensive care unit patients: a randomized controlled study
- PMID: 20426859
- PMCID: PMC2887199
- DOI: 10.1186/cc8989
A recruitment maneuver increases oxygenation after intubation of hypoxemic intensive care unit patients: a randomized controlled study
Abstract
Introduction: Tracheal intubation and anaesthesia promotes lung collapse and hypoxemia. In acute lung injury patients, recruitment maneuvers (RMs) increase lung volume and oxygenation, and decrease atelectasis. The aim of this study was to evaluate the efficacy and safety of RMs performed immediately after intubation.
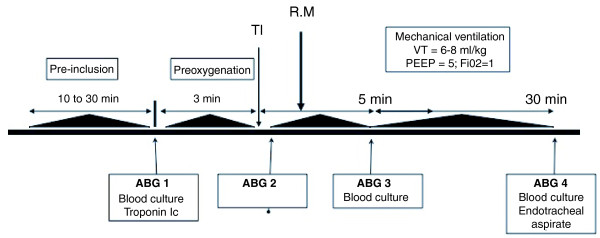
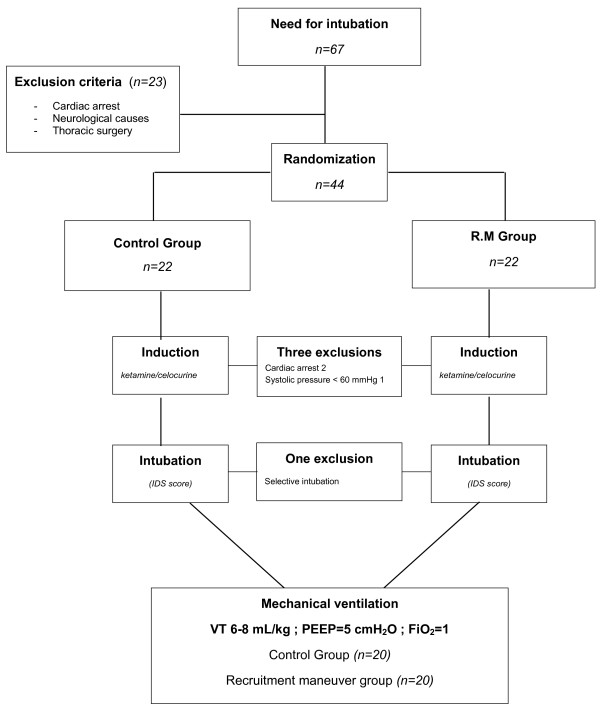
Methods: This randomized controlled study was conducted in two 16-bed medical-surgical intensive care units within the same university hospital. Consecutive patients requiring intubation for acute hypoxemic respiratory failure were included. Patients were randomized to undergo a RM immediately (within 2 minutes) after intubation, consisting of a continuous positive airway pressure (CPAP) of 40 cmH2O over 30 seconds (RM group), or not (control group). Blood gases were sampled and blood samples taken for culture before, within 2 minutes, 5 minutes, and 30 minutes after intubation. Haemodynamic and respiratory parameters were continuously recorded throughout the study. Positive end expiratory pressure (PEEP) was set at 5 cmH2O throughout.
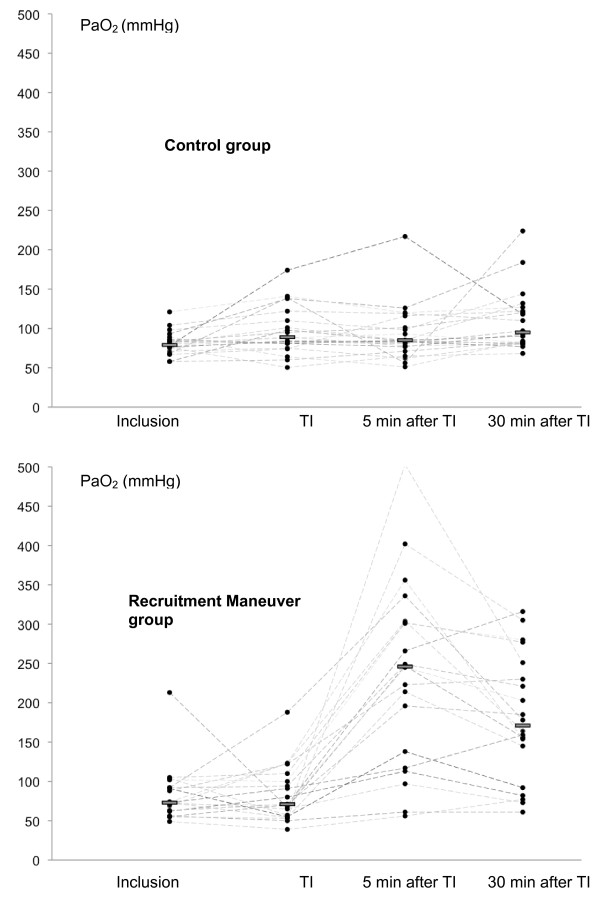
Results: The control (n = 20) and RM (n = 20) groups were similar in terms of age, disease severity, diagnosis at time of admission, and PaO2 obtained under 10-15 L/min oxygen flow immediately before (81 +/- 15 vs 83 +/- 35 mmHg, P = 0.9), and within 2 minutes after, intubation under 100% FiO2 (81 +/- 15 vs 83 +/- 35 mmHg, P = 0.9). Five minutes after intubation, PaO2 obtained under 100% FiO2 was significantly higher in the RM group compared with the control group (93 +/- 36 vs 236 +/- 117 mmHg, P = 0.008). The difference remained significant at 30 minutes with 110 +/- 39 and 180 +/- 79 mmHg, respectively, for the control and RM groups. No significant difference in haemodynamic conditions was observed between groups at any time. Following tracheal intubation, 15 patients had positive blood cultures, showing microorganisms shared with tracheal aspirates, with no significant difference in the incidence of culture positivity between groups.
Conclusions: Recruitment maneuver following intubation in hypoxemic patients improved short-term oxygenation, and was not associated with increased adverse effects.
Trial registration: NCT01014299.
Figures
Comment in
-
Do recruitment maneuvers simply improve oxygenation?Crit Care. 2010;14(4):173. doi: 10.1186/cc9042. Epub 2010 Jul 1. Crit Care. 2010. PMID: 20598114 Free PMC article.
References
-
- Hedenstierna G. Pulmonary perfusion during anesthesia and mechanical ventilation. Minerva Anestesiol. 2005;71:319–324. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
