

Epidemiologic relationships between A1C and all-cause mortality during a median 3.4-year follow-up of glycemic treatment in the ACCORD trial
- PMID: 20427682
- PMCID: PMC2858202
- DOI: 10.2337/dc09-1278
Epidemiologic relationships between A1C and all-cause mortality during a median 3.4-year follow-up of glycemic treatment in the ACCORD trial
Abstract
Objective: Randomized treatment comparing an intensive glycemic treatment strategy with a standard strategy in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial was ended early because of an unexpected excess of mortality in the intensive arm. As part of ongoing post hoc analyses of potential mechanisms for this finding, we explored whether on-treatment A1C itself had an independent relationship with mortality.
Research design and methods: Participants with type 2 diabetes (n = 10,251 with mean age 62 years, median duration of diabetes 10 years, and median A1C 8.1%) were randomly assigned to treatment strategies targeting either A1C <6.0% (intensive) or A1C 7.0-7.9% (standard). Data obtained during 3.4 (median) years of follow-up before cessation of intensive treatment were analyzed using several multivariable models.
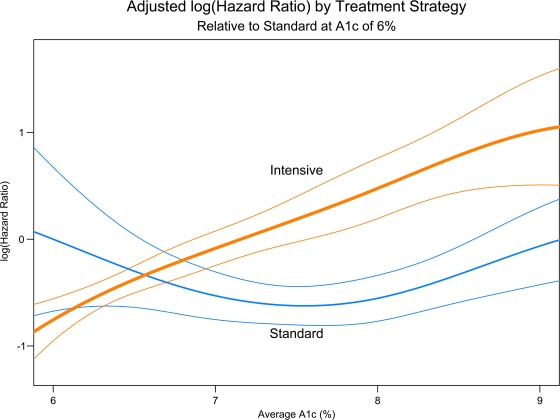
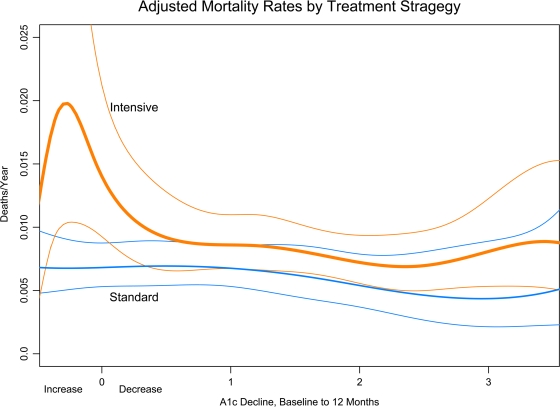
Results: Various characteristics of the participants and the study sites at baseline had significant associations with the risk of mortality. Before and after adjustment for these covariates, a higher average on-treatment A1C was a stronger predictor of mortality than the A1C for the last interval of follow-up or the decrease of A1C in the first year. Higher average A1C was associated with greater risk of death. The risk of death with the intensive strategy increased approximately linearly from 6-9% A1C and appeared to be greater with the intensive than with the standard strategy only when average A1C was >7%.
Conclusions: These analyses implicate factors associated with persisting higher A1C levels, rather than low A1C per se, as likely contributors to the increased mortality risk associated with the intensive glycemic treatment strategy in ACCORD.
Trial registration: ClinicalTrials.gov NCT00000620.
Figures
Comment in
-
ACCORD glycemia results continue to puzzle.Diabetes Care. 2010 May;33(5):1149-50. doi: 10.2337/dc10-0432. Diabetes Care. 2010. PMID: 20427688 Free PMC article. No abstract available.
References
-
- Kannel WB, McGee DL: Diabetes and cardiovascular disease: the Framingham study. JAMA 1979; 241: 2035– 2038 - PubMed
-
- Stamler J, Vaccaro O, Neaton JD, Wentworth D: Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the Multiple Risk Factor Intervention Trial. Diabetes Care 1993; 16: 434– 444 - PubMed
-
- Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M: Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 1998; 339: 229– 234 - PubMed
-
- Wei M, Gaskill SP, Haffner SM, Stern MP: Effects of diabetes and level of glycemia on all-cause and cardiovascular mortality. The San Antonio Heart Study. Diabetes Care 1998; 21: 1167– 1172 - PubMed
-
- Coutinho M, Gerstein HC, Wang Y, Yusuf S: The relationship between glucose and incident cardiovascular events: a meta regression analysis of published data from 20 studies of 95,783 individuals followed for 12.4 years. Diabetes Care 1999; 22: 233– 240 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- N01 HC095179/HL/NHLBI NIH HHS/United States
- N01 HC095184/HL/NHLBI NIH HHS/United States
- N01-HC-95180/HC/NHLBI NIH HHS/United States
- N01 HC095178/HL/NHLBI NIH HHS/United States
- N01-HC-95184/HC/NHLBI NIH HHS/United States
- IAA-Y1-HC-1010/HC/NHLBI NIH HHS/United States
- N01 HC095182/HL/NHLBI NIH HHS/United States
- N01-HC-95183/HC/NHLBI NIH HHS/United States
- N01-HC-95178/HC/NHLBI NIH HHS/United States
- N01-HC-95179/HC/NHLBI NIH HHS/United States
- N01-HC-95181/HC/NHLBI NIH HHS/United States
- IAA-Y1-HC-9035/HC/NHLBI NIH HHS/United States
- N01 HC095180/HL/NHLBI NIH HHS/United States
- Y01 HC001010/HC/NHLBI NIH HHS/United States
- Y01 HC009035/HC/NHLBI NIH HHS/United States
- N01 HC095181/HL/NHLBI NIH HHS/United States
- N01-HC-95182/HC/NHLBI NIH HHS/United States
- N01 HC095183/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
