

Renal histopathology and crystal deposits in patients with small bowel resection and calcium oxalate stone disease
- PMID: 20428098
- PMCID: PMC3787699
- DOI: 10.1038/ki.2010.131
Renal histopathology and crystal deposits in patients with small bowel resection and calcium oxalate stone disease
Abstract
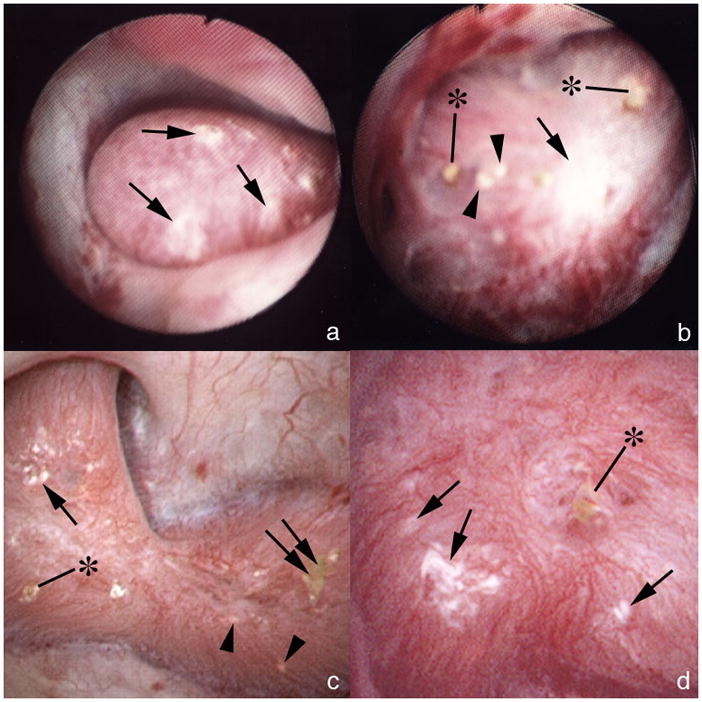
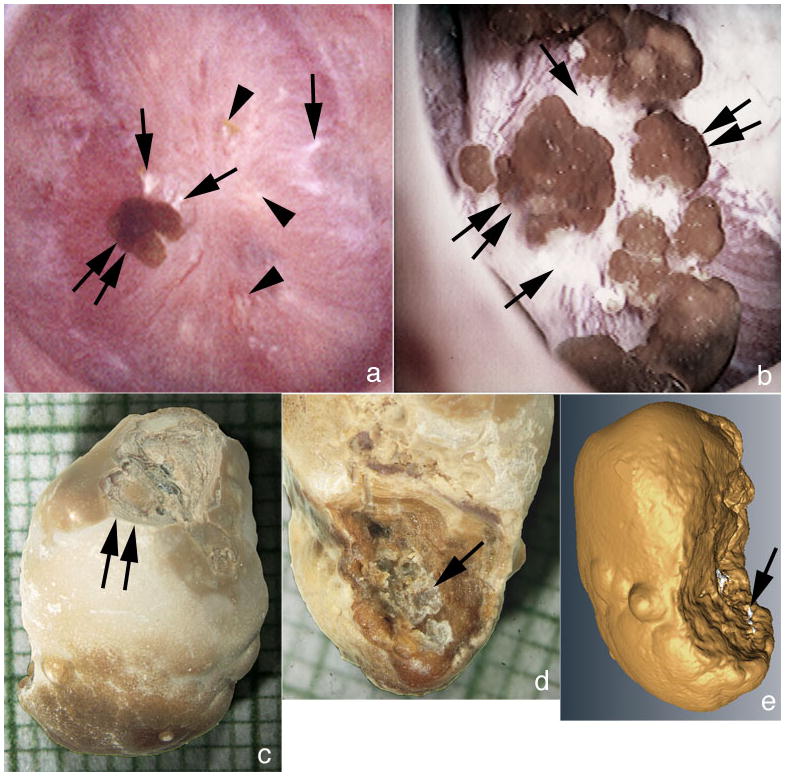
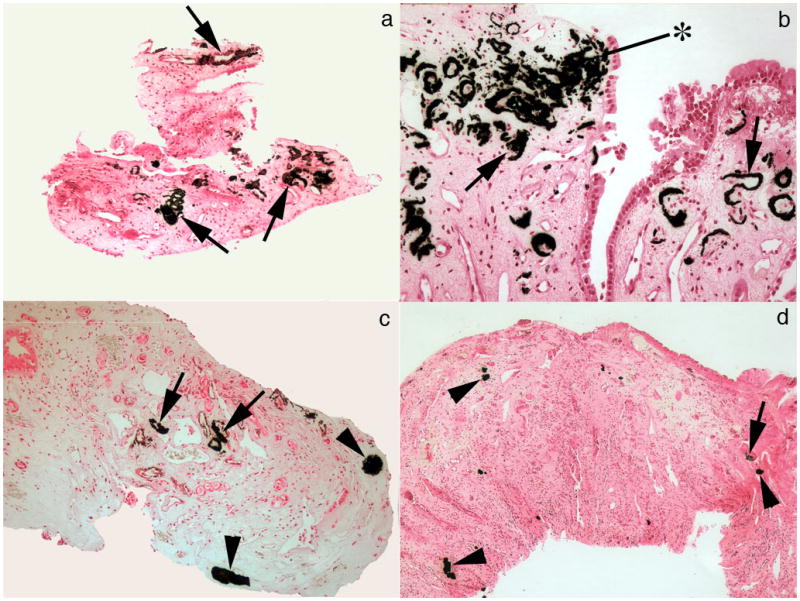
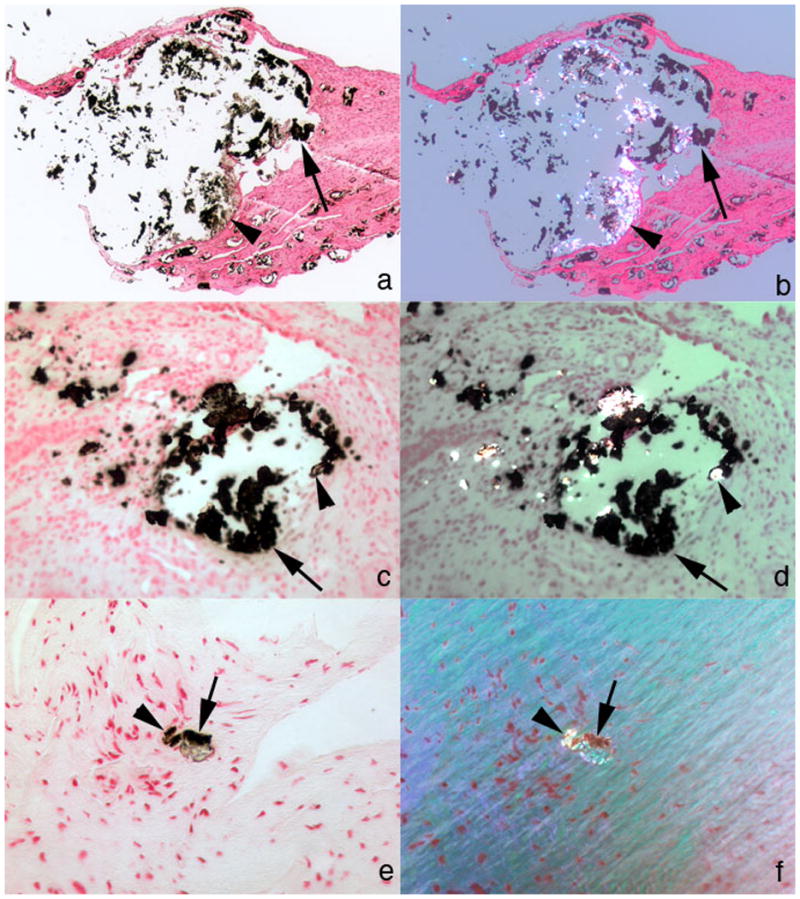
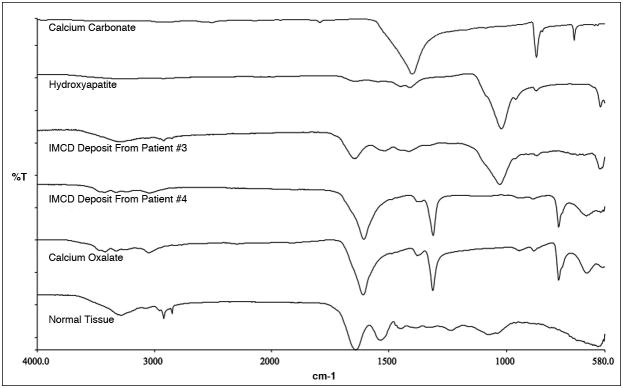
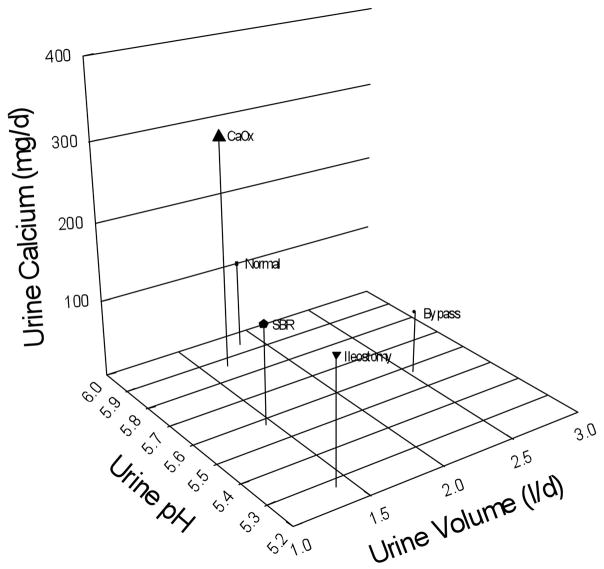
We present here the anatomy and histopathology of kidneys from 11 patients with renal stones following small bowel resection, including 10 with Crohn's disease and 1 resection in infancy for unknown cause. They presented predominantly with calcium oxalate stones. Risks of formation included hyperoxaluria (urine oxalate excretion greater than 45 mg per day) in half of the cases, and acidic urine of reduced volume. As was found with ileostomy and obesity bypass, inner medullary collecting ducts (IMCDs) contained crystal deposits associated with cell injury, interstitial inflammation, and papillary deformity. Cortical changes included modest glomerular sclerosis, tubular atrophy, and interstitial fibrosis. Randall's plaque (interstitial papillary apatite) was abundant, with calcium oxalate stone overgrowth similar to that seen in ileostomy, idiopathic calcium oxalate stone formers, and primary hyperparathyroidism. Abundant plaque was compatible with the low urine volume and pH. The IMCD deposits all contained apatite, with calcium oxalate present in three cases, similar to findings in patients with obesity bypass but not an ileostomy. The mechanisms for calcium oxalate stone formation in IMCDs include elevated urine and presumably tubule fluid calcium oxalate supersaturation, but a low calcium to oxalate ratio. However, the mechanisms for the presence of IMCD apatite remain unknown.
Conflict of interest statement
Disclosure:
All the authors declared no competing interests.
Figures
References
-
- Evan AP, Coe FL, Gillen D, et al. Renal intratubular crystals and hyaluronan staining occur in stone formers with bypass surgery but not with idiopathic calcium oxalate stones. Anat Rec (Hoboken) 2008;291:325–334. - PubMed
-
- Evan AE, Lingeman JE, Coe FL, et al. Histopathology and surgical anatomy of patients with primary hyperparathyroidism and calcium phosphate stones. Kidney Int. 2008;74:223–229. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
